Tracheomegaly
Martha Huller Maier, MD
Key Facts
Terminology
Dilatation of trachea and central bronchi with relatively abrupt transition to normal caliber of peripheral airways
Imaging Findings
Trachea and 1st- through 4th-order bronchi affected
Diagnosis often overlooked
Men: Tracheal transverse diameter > 25 mm, sagittal diameter > 27 mm
Women: Tracheal transverse diameter > 21 mm, sagittal diameter > 23 mm
CT: Dilatation may also be overlooked
Hint: Trachea may be bigger than ascending aorta
Top Differential Diagnoses
Sarcoidosis
Allergic Bronchopulmonary Aspergillosis
Cystic Fibrosis
Saber-Sheath Trachea
Relapsing Polychondritis
Pathology
Most cases considered congenital, but true etiology unknown
Clinical Issues
Presentation variable: Asymptomatic to severe respiratory symptoms
More common in 3rd or 4th decades
Rarely diagnosed in infancy or childhood even though considered congenital
Smoking cessation extremely important
Conservative treatment: Chest physiotherapy to clear secretions and antibiotics for infections
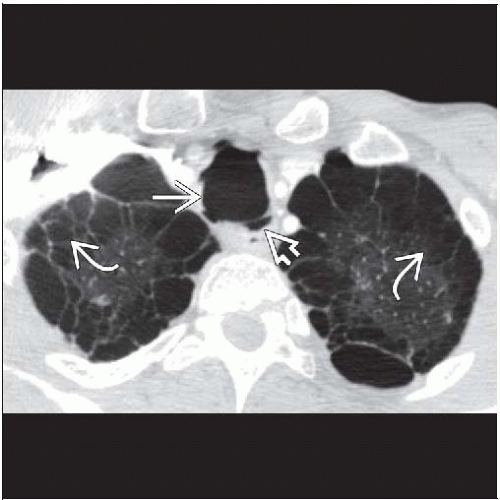 Axial CECT shows an enlarged trachea  and multiple tracheal diverticula and multiple tracheal diverticula  . Paraseptal emphysema . Paraseptal emphysema  is also extensive. is also extensive. |
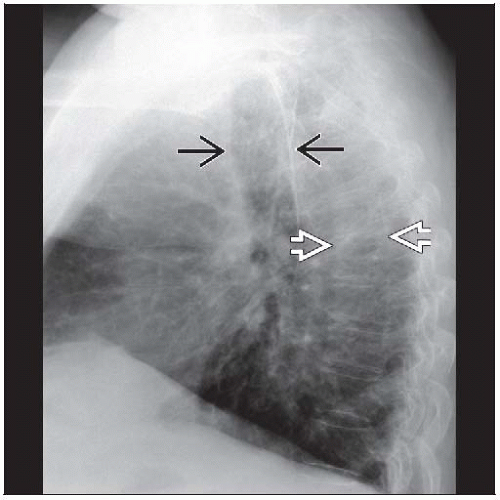 Lateral radiograph shows the typical radiographic features of a dilated trachea (28 mm) due to tracheobronchomegaly  . The trachea is as wide as the vertebral bodies . The trachea is as wide as the vertebral bodies  . . |
TERMINOLOGY
Abbreviations and Synonyms
Mounier-Kuhn syndrome, trachiectasis, megatrachea, tracheobronchiectasis, tracheocele, tracheobronchopathia malacia
Definitions
Dilatation of trachea and central bronchi with relatively abrupt transition to normal caliber of peripheral airways
IMAGING FINDINGS
General Features
Best diagnostic clue
Enlarged luminal diameter of trachea and central bronchi
Tracheal diverticulosis: Irregular, corrugated, scalloped, or undulating appearance of trachea
Often overlooked on radiographs or CT
Patient position/location
Trachea and 1st- through 4th-order bronchi affected
May extend as high as the larynx
Airways distal to 4th- and 5th-order bronchi usually normal in diameter
Exception: Repeated infection associated with the disease may eventually lead to distal bronchiectasis
Size
Women: Tracheal transverse diameter > 21 mm, sagittal diameter > 23 mm
Transverse diameter right mainstem bronchus > 19.8 mm, left mainstem bronchus > 17.4 mm
Men: Tracheal transverse diameter > 25 mm, sagittal diameter > 27 mm
Transverse diameter right mainstem bronchus > 21.1 mm, left mainstem bronchus > 18.4 mm
Measurements reflect 3 standard deviations above the mean
Morphology
Diffuse luminal enlargement of affected airways
Airway walls are thinned, atrophic, and abnormally weak
Tracheal diverticulosis due to
Muscular and elastic atrophy in cartilaginous and membranous portions of trachea and bronchi
Mucosa, submucosa herniate between tracheal ring causing protrusions ranging in size from several mm to cm
Bronchoscope may easily enter these herniations
Pooled secretions may give rise to chronic infection
CT Findings
NECT: Easy and accurate visualization and measurement of tracheal diameter
HRCT
For improved visualization of abnormally thinned, atrophic walls of affected airways
More sensitive for associated abnormalities
Tracheal diverticula: Most often originate from right posterolateral wall
Diverticula may be fluid filled or have air-fluid levels (contributed to chronic infection and aspiration)Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



