Trauma
Sathish Kumar Dundamadappa
David Choi
Aly H. Abayazeed
Shyam Sabat
Prachi Dubey
QUESTIONS
1 A 45-year-old male, unrestrained passenger brought to the ER after a high-speed motor vehicle accident.
|

1a What is the most likely diagnosis?
A. Subdural hematoma
B. Subdural empyema
C. Epidural hematoma
D. Epidural metastasis
1b Venous epidural hematomas are commonly associated with injury to what structure?
A. Dural venous sinus
B. Middle meningeal vein
C. Deep cerebral veins
D. Emissary veins
View Answer
1b Answer A. Dural venous sinus.
|

Imaging Findings: A lenticular predominantly hyperattenuating extra-axial collection with swirling intermixed iso- to hypoattenuating components. On bone windows, there is a nondisplaced fracture of the right parietal bone coursing anterior to the lambdoid suture. Findings are compatible with an acute epidural hematoma.
Discussion: Epidural hematomas are most commonly from arterial origin, resulting from injury to the meningeal arteries, typically the middle meningeal artery. These are bounded by dural attachments at the sutures and majority of these (>80%) are associated with skull fractures. Rarely, these may be seen without a fracture, usually in pediatric age group because of shearing or stretching of meningeal vessels. Venous epidural hematomas are relatively rare and typically seen with injury to dural venous sinuses.
Reference: Atlas SW. Head Trauma. In: Magnetic resonance imaging of the brain and spine, 4th ed. Vol. 1. Chap. 17. Lippincott Williams & Wilkins, 917-918.
2 A 38-year-old male presents to the ER after MVA. She has fractured bilateral pterygoid plates on CT.
|

Based on the above appearance, which of the following best classifies this pattern of injury?
A. Le Fort I
B. Le Fort II
C. Le Fort III
D. Le Fort VI
View Answer
2 Answer A. Le Fort I.
|

Imaging Findings: Axial and coronal noncontrast CT demonstrates fractures involving the pterygomaxillary junction and plates and fracture of inferior medial and lateral maxillary buttress.
Discussion: Le Fort 1 fracture. Multidetector computed tomography (CT) is the modality of choice for the evaluation of facial trauma because it helps accurately identify and characterize fractures. In particular, CT clearly depicts clinically relevant fractures in the eight osseous struts or buttresses that provide a scaffold for facial structures. Analyses of specific facial buttresses in a complex fracture aid determining the type of fracture and associated soft tissue injuries that may require urgent care or surgery.
Le Fort fractures are complex facial fractures that result from a high-force impact on the midface and are characterized by a variable degree of craniofacial dissociation spanning multiple facial buttresses. These fractures were first described in early 20th century by French surgeon René Le Fort, who conducted experiments applying blunt force to midface of cadavers.
Le Fort type I fracture, also known as “floating palate,” results in separation of the hard palate (fracture of the medial and lateral horizontal maxillary buttresses and separation of the lower transverse maxillary buttress) from the remainder of the face and the skull base. This fracture pattern is horizontally oriented and spans the anterior, lateral, and medial maxillary walls, transecting the inferior margin of the piriform aperture and nasal septum and extending posteriorly through the pterygoid plates. The fractures are usually best depicted on coronal and three-dimensional images.
Long-term complications of Le Fort type I fracture may include malocclusion, mastication problems, facial deformity, and breathing difficulty, among others.
References: Chung KJ, et al. Treatment of complex facial fractures: clinical experience of different timing and order. J Craniofac Surg 2013;24(1):216-220.
Lo Casto A, et al. Imaging evaluation of facial complex strut fractures. Semin Ultrasound CT MR 2012;33(5):396-409.
Winegar BA, et al. Spectrum of critical imaging findings in complex facial skeletal trauma. Radiographics 2003;33(1):3-19.
3 Based on the progressive CT scan appearance shown below in a recently postoperative patient, what is the most likely diagnosis?
|

A. Extracranial herniation postcraniectomy
B. Sinking skin flap syndrome
C. Progressive postoperative encephalomalacia
D. Tension pneumocephalus
View Answer
3 Answer B. Sinking skin flap syndrome. There is a right-sided craniectomy with the skin flap collapsing inward in a paradoxical fashion. No evidence of postop encephalomalacia or tension pneumocephalus seen on these images.
|

Imaging Findings: Right-sided craniectomy (A) with progressively sinking flap (B and C) and compression of right lateral ventricle (C).
Discussion: Sinking skin flap syndrome or trephined syndrome. It is a rare delayed complication after craniectomy associated with neurologic deterioration that resolves after a cranioplasty. Instead of extracranial herniation as intended by the decompression craniectomy to decompress the central structures, there is “paradoxical” herniation as a consequence of atmospheric pressure exceeding intracranial pressure. The underlying etiology is unclear and could be related to alteration in CSF physiology.
Radiologically, there can be presence of sunken skin flap, shift of midline structures, and lower 3rd ventricle and relative intracranial CSF volumes. Clinically, these patients may have headache, fatigability, tinnitus, discomfort at the site of the defect, depression, intolerance to vibration, and cognitive impairment. The presence of sunken skin flap itself, as shown in this case, is the most common radiologic sign associated with the clinical syndrome of trephined but is not a prerequisite for developing this condition. The second most common sign is paradoxical herniation, that is, shift of midline structures away from the craniectomy defect. Timely recognition of this entity is critical for early intervention that can significantly enhance patient outcomes.
References: Annan M, De Toffol B, Hommet C, et al. Sinking skin flap syndrome (or syndrome of the trephined): a review. Br J Neurosurg 2015;29(3):314-318.
Vasung L, Hamard M, Soto MC, et al. Radiological signs of the syndrome of the trephined. Neuroradiology 2016;58(6):557-568.
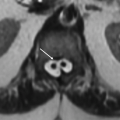
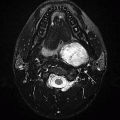
4 A 4-year-old female with right ICA dissection, following a reported fall. Head CT and MRI were performed as a part of the workup. Key images are shown below.
|

4a Additional radiographs are being performed as a part of the workup. Based on this study, what additional evaluation should be recommended?
A. Indirect ophthalmoscopy with dilated pupils
B. 24-hour EEG monitoring
C. Muscle biopsy for mitochondrial disorders
D. MRI brain with contrast
View Answer
4a Answer A. Indirect ophthalmoscopy with dilated pupils. There is right hemispheric infarction and presence of high density abutting the retina in the right globe suggesting hemorrhage. This raises concern for nonaccidental injury and dedicated ophthalmoscopy for detailed assessment of retinal hemorrhages, pattern, and extent should be performed for both eyes. Note lower sensitivity of CT for retinal hemorrhage; therefore, careful evaluation of the left eye is also necessary despite no obvious abnormality on CT. Most instances of nonaccidental injury have bilateral involvement, which is more extensive and has foci that extend to the periphery.
4b What is the reported probability of abuse in a child with head trauma and retinal hemorrhages?
A. 90%
B. 10% to 15%
C. 30%
D. <10%
View Answer
4b Answer A. 90%. Based on a published review, 91% probability of abuse has been reported in patients with head trauma and retinal hemorrhage (Maguire et al., 2013, reference below). Others report this range can be from 50% to 100%, so of the available choices the best answer would be A.
|

Imaging Findings: Presence of high-density focus abutting the retina in the right eye, suspicious for retinal hemorrhage (A) with right hemispheric restricted diffusion compatible with right ICA infarction in the setting of right ICA dissection.
Discussion: Retinal hemorrhage (RH) is a major factor associated with nonaccidental injury (NAI). The probability of abuse in children with head injury and RH has found to be as high as 91%. A thorough ophthalmologic evaluation with a dilated pupil is necessary for better assessment whenever abuse is suspected. RH in NAI is usually bilateral, multilayered, and extensive with peripheral involvement. Other noninflicted entities such as severe crush injuries or high-altitude fall can rarely have an overlapping appearance; therefore, careful assessment of history, clinical features, and other signs of inflicted injury in consultation with multidisciplinary specialists is necessary.
Differential possibilities, such as elevated intracranial pressure, result in relatively superficial intraretinal hemorrhage. Terson syndrome, which is associated with subarachnoid hemorrhage such as from an aneurysmal rupture, is characterized by preretinal and vitreous hemorrhage, unlike NAI, which has intraretinal hemorrhages.
References: Binenbaum G, Forbes BJ. The eye in child abuse: key points on retinal hemorrhages and abusive head trauma. Pediatr Radiol 2014;44(Suppl 4):S571-S577.
Maguire SA, Watts PO, Shaw AD, et al. Retinal haemorrhages and related findings in abusive and non-abusive head trauma: a systematic review. Eye (Lond) 2013;27(1):28-36.
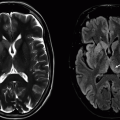
5 Key images from an MRI performed for evaluation of an abnormal head CT are shown below.
|

5a What are the lesions indicated by arrows in image A?
A. Metastatic lesions
B. Hemorrhagic contusions
C. Multifocal embolic infarcts
D. Septic emboli with abscess
View Answer
5a Answer B. Hemorrhagic contusions. Location (anteroinferior frontal lobes and lateral temporal lobe) and associated hemorrhage are typical for traumatic hemorrhagic contusions.
5b Which of the following statements is accurate regarding traumatic brain contusions?
A. Commonly enlarge over first 2 days following causative event.
B. Consistently seen on immediate posttrauma imaging.
C. Caused by shear injury.
D. CT is more sensitive than MRI for detection of these abnormalities.
View Answer
5b Answer A. Commonly enlarge over first 2 days following causative event. Though contusions are considered primary injury, increase in number and size is commonly seen within first 48 hours following trauma. These are “brain bruises” resulting from impact of the moving brain against fixed bones/dura. MRI is much more sensitive than CT, especially for small lesions.
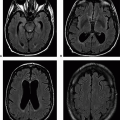
5c A key image from T2 FLAIR sequence obtained in the same patient is shown below.
|

Which of the following abnormality is indicated by arrows in the above image?
A. Subarachnoid hemorrhage
B. Pial collateral vessels, indicating vascular occlusion
C. Leptomeningeal carcinomatosis
D. Superficial cortical veins, normal finding
View Answer
5c Answer A. Subarachnoid hemorrhage. The other choices are differential considerations for signal abnormality in subarachnoid space on FLAIR images. But given the presence of contusions, the appearance likely represents subarachnoid hemorrhage.
|

Imaging Findings: Hemorrhagic lesions showing some diffusion restriction present in inferior medial frontal lobes and lateral right temporal lobe, consistent with hemorrhagic contusions (A, B, and C). Scattered FLAIR hyperintense signal in subarachnoid spaces, left more than right, consistent with subarachnoid hemorrhage (D).
Discussion: Traumatic contusions and subarachnoid hemorrhage
Contusions:
Contusions are the most common parenchymal injury with head trauma.
Based on the mechanism, they can be classified as coup contusions (at the site of direct impact) and contrecoup contusions (injury distant to the area of direct impact).
Parasagittal contusions are known as “gliding contusions” caused by angular acceleration with impact of the brain against falx and bone occurring over parasagittal convexity. Less common, “fracture contusions” are due to direct injury to brain parenchyma from fracture fragments.
Given the mechanism, they tend to occur in typical locations—inferomedial frontal lobes, frontal tips, anterior temporal lobes, lateral temporal lobes, and parasagittal convexity. They are often bilateral. Though this is a primary injury, nearly half of the patients reveal contusions on imaging over first 48 hours.
On CT scans, contusions are seen as hyperdense hemorrhages and surrounding edema. Immediately following trauma, smaller contusions may not be well seen on CT. A characteristic “salt-and-pepper” appearance is more apparent in follow-up scans with hyperdense hemorrhages and increasing surrounding edema.
MRI is more sensitive for contusions than CT. Hemorrhages bloom on gradient-or susceptibility-weighted images and surrounding edema is easily seen on FLAIR-/T2-weighted images. Edema associated with contusions can increase up to a week. Occasionally, contusions can be nonhemorrhagic.
Subarachnoid hemorrhage:
Subarachnoid hemorrhage is the most common extra-axial hemorrhage following trauma.
CT, which is in the modality of choice for evaluation of trauma, is highly sensitive of subarachnoid hemorrhage in acute setting. If the SAH is very small, it may quickly become less apparent on CT because of dilution and distribution. CT is not very sensitive for SAH in subacute state.
MRI FLAIR sequence is probably equally sensitive or perhaps more sensitive than CT for subarachnoid hemorrhage in acute setting. However, it is nonspecific. Other etiologies for FLAIR hyperintensity along the sulci need to be excluded. In subacute phase, FLAIR- and susceptibility-weighted imagings are much more sensitive than CT. In chronic stage, hemosiderin staining of meningitis is demonstrated on gradient- or susceptibility-weighted images.
References: Gean AD, Fischbein NJ. Head trauma. Neuroimaging Clin N Am 2010;20(4):527-556.
Naidich TP, ed. Imaging of the brain. Expert Radiology Series. Philadelphia, PA: Saunders/Elsevier, 2013.
van Gijn J, Kerr RS, Rinkel GJ. Subarachnoid haemorrhage. Lancet 2007;369(9558):306-318.
6 A 40-year-old patient sustained blunt trauma to the face. Key images from CT are shown below.
|

What is the most likely diagnosis?
A. Le Fort type III fracture
B. Zygomaticomaxillary complex fracture
C. Orbital blowout fracture
D. Nasoorbitoethmoidal fracture
View Answer
6 Answer C. Orbital blowout fracture.
|

Imaging Findings: There is an isolated fracture fragment of the orbital floor displaced into the maxillary sinus with herniation of orbital contents, consistent with orbital floor blowout fracture.
Discussion: The orbital blowout fracture, typically of the orbital floor or medial wall, is caused by a sudden increase in intraorbital pressure from a blunt force such as a fist. Le Fort fractures disconnect portions of the face from the cranium, with pterygoid plate disruption the common denominator for all Le Fort fractures. Zygomaticomaxillary fractures disrupt the zygomaticofrontal, zygomaticomaxillary, zygomaticosphenoidal, and zygomaticotemporal sutures. The nasoorbitoethmoidal fracture comprises depressed fractures of the nasal bones, medial maxillary buttresses including the medial orbital walls, and ethmoid sinuses.
Although entrapment of the extraocular muscles can be suspected based on imaging, entrapment must be confirmed by clinical testing. Entrapment is a clinical, not an imaging diagnosis.
References: Oppenheimer AJ, Monson LA, Buchman SR. Pediatric orbital fractures. Craniomaxillofac Trauma Reconstr 2013;6(1):9-20.
Winegar BA, Murillo H, Tantiwongkosi B. Spectrum of critical imaging findings in complex facial skeletal trauma. Radiographics 2013;33(1):3-19.
7 A 30-year-old male was brought to the ER after motor vehicle accident. Key CT and MR images are shown below.
|

7a What is the most likely diagnosis?
A. Hypoxic ischemic encephalopathy
B. Diffuse axonal injury
C. Multifocal embolic infarcts because of fat embolism
D. Hypertensive hemorrhages
7b A common location of microhemorrhages in mild forms of DAI is:
A. Gray-white interface
B. Choroid plexus
C. Thalamus
D. Dorsolateral brainstem
View Answer
7b Answer A. Gray-white interface.
|

Imaging Findings: CT, FLAIR and susceptibility-weighted MR images show intraventricular hemorrhage (dotted arrow, A) and multiple small foci of parenchymal hemorrhage and edema, distributed in subcortical and deep white matter, basal ganglia, and corpus callosum (arrows D, E and F). There are foci of petechial hemorrhage, many associated with bright signal on the DWI images (arrows B and C). The constellation of findings is most consistent with diffuse axonal injury.
Discussion: Diffuse axonal injury reflects predominantly shear injury to axons, most of which is beyond the resolution of conventional MR imaging. With mild cases of diffuse axonal injury, the most commonly affected sites are at gray-white interfaces. Deeper brain structures are increasingly involved with more severe injury, including basal ganglia, thalamus, brainstem, within ventricles, and choroid plexus.
References: Koerte IK, Hufschmidt J, Muehlmann M, et al. Advanced neuroimaging of mild traumatic brain injury. In: Laskowitz D, Grant G. (eds). Translational research in traumatic brain injury. Boca Raton, FL: CRC Press/Taylor and Francis Group, 2016. Chapter 13. Frontiers in Neuroscience.
Provenzale JM. Imaging of traumatic brain injury: a review of the recent medical literature. AJR Am J Roentgenol 2010;194(1):16-19.
8 Patient presents with acute headache and confusion. Noncontrast head CT was performed. Key images are shown below.
|

What is the most likely diagnosis?
A. No abnormality shown on provided images
B. Venous epidural hematoma
C. Idiopathic intracranial hypertension
D. Subdural hematoma
View Answer
8 Answer D. Subdural hematoma. There is a left hemispheric subdural hematoma that is nearly isoattenuating to gray matter.
|

Imaging Findings: There is effacement of sulci of the left cerebral hemisphere. Closer inspection reveals a large crescentic extra-axial abnormality, nearly isodense to brain parenchyma in the left frontal and parietal regions. The abnormality crosses the expected location of the coronal suture. The findings most likely reflect an isodense subdural hematoma.
Discussion: The density of subdural hematoma may be diffusely isodense relative to brain parenchyma in several circumstances, including the subacute stage, from blood mixed with CSF, during anemia, and disseminated intravascular coagulation.
In the early subacute stage, subdural hematoma largely comprises intracellular methemoglobin, which has both T1 shortening and T2 shortening effects, which can lead to hyperintense signal on T1-weighted images, hypointense signal on T2-weighted images, and hypointense signal on FLAIR images. In the late subacute stage, lysis of the RBC leads to extracellular methemoglobin, which prolongs T2 and shortens T1, with resultant hyperintense signal on T1-weighted images, T2-weighted images, and FLAIR images.
Acute subdural hematoma is typically hyperdense but may be isodense in anemia, DIC, or hemorrhage mixed with CSF. Mixed density acute subdural hematoma may occur in setting of active bleeding (hyperacute hemorrhage is isointense), CSF mixing with hemorrhage, and retraction of clot.
References: Gandhoke GS, Kaif M, Choi L, et al. Histopathological features of the outer membrane of chronic subdural hematoma and correlation with clinical and radiological features. J Clin Neurosci 2013;20(10):1398-1401.
Wilms G, Marchal G, Geusens E, et al. Isodense subdural haematomas on CT: MRI findings. Neuroradiology 1992;34(6):497-499.

A. Comminuted nasal fracture
B. Nasoorbitoethmoidal (NOE) fracture
C. Le Fort type III (transfacial) fracture
D. Bilateral medial orbital blowout fractures
9b What clinical sign would distinguish this fracture pattern from bilateral medial orbital blowout fractures?
A. Hyphema
B. Monocular loss of vision
C. Telecanthus
D. Periorbital crepitus
View Answer
9b Answer C. Telecanthus.
|

Imaging Findings: There is a comminuted depressed fracture through the nasal bones and underlying ethmoid air cells, with disruption of the superior aspect of the medial maxillary buttresses bilaterally, including the medial orbital walls, characteristic of nasoorbitoethmoidal fractures.
Discussion: In nasoorbitoethmoidal fractures, the attachment of the medial canthal ligaments is often disrupted, leading to telecanthus.
Other potential complications include epiphora from nasolacrimal apparatus injury, ocular injury with blindness, disruption of frontal sinus drainage, CSF leak, meningitis, and meningoencephalocele. The disruption of the medial orbital walls and ethmoids distinguishes this fracture pattern from isolated nasal bone fractures.
The Le Fort type III fracture, or craniofacial dissociation, involves the lateral maxillary and upper horizontal maxillary buttresses and zygomatic arches in addition to the medial maxillary buttresses. Isolated orbital blowout fractures typically involve the orbital floor or lamina papyracea.
Isolated orbital blowout fractures do not involve the orbital rim and thus would unlikely disrupt the medial canthal tendon. Hyphema, monocular loss of vision, and oculocardiac reflex (bradycardia induced by traction on extraocular muscles or pressure on the globes) may occur in both NOE and orbital blowout fractures. Periorbital crepitus typically from the sinonasal region fractures are also not specific to either fracture pattern.
Nasoorbitoethmoidal fractures may disrupt the cribriform plate or the frontal sinuses, posing risk of CSF leak, meningitis, and meningoencephalocele.
References: Hopper RA, Salemy S, Sze RW. Diagnosis of midface fractures with CT: what the surgeon needs to know. Radiographics 2006;26(3):783-793.
Winegar BA, Murillo H, Tantiwongkosi B. Spectrum of critical imaging findings in complex facial skeletal trauma. Radiographics 2013;33(1):3-19.

A. Zygomatic arch fracture
B. Orbital floor blowout fracture
C. Le Fort type II fracture
D. Zygomaticomaxillary complex fracture
10b What neurologic sign is most specifically associated with this fracture pattern?
A. Diplopia
B. Anesthesia cheek/upper lip
C. Monocular visual loss
D. Ipsilateral sensorineural hearing loss
View Answer




10b Answer B. Anesthesia cheek/upper lip.
|

Imaging Findings: Fractures of anterior maxillary wall, zygomatic arch, lateral orbital wall, and orbital floor are shown above (A, B, C). Fractures in this case disrupt the zygomaticofrontal, zygomaticomaxillary, zygomaticosphenoidal, and zygomaticotemporal sutures. This pattern is characteristic of zygomaticomaxillary complex fractures.
Discussion: Tripod fracture (more accurately, tetrapod or quadripod fracture) is generally caused by a direct blow to the cheek. It is also known as zygomaticomaxillary complex fracture, which is generally the preferred terminology.
Zygomatic bone forms lateral orbital rim inferior to zygomatic process of the frontal bone, the lateral orbital wall anterior to the sphenoid, the anterior and lateral maxillary sinus walls superior to the hard palate, and the zygomatic arch anterior to temporal bone. It is connected to rest of the facial skeleton and calvarium by four sutures—zygomaticofrontal suture, zygomaticomaxillary suture, zygomaticotemporal suture, and zygomaticosphenoid suture.
Zygomaticomaxillary complex fracture refers to fractures involving anterior and posterolateral maxillary sinus walls, orbital floor, lateral orbital wall, and zygomatic arch, fracture lines coursing through or near the abovementioned four sutures with resultant separation of the zygoma from the calvarium and remainder of the facial skeleton. In radiographs, the zygomaticosphenoid suture fracture is not well demonstrated and only fractures through the other three sutures can be demonstrated and hence the older terminology “tripod fracture.” Rotational forces by masseter muscle can displace the fractured zygoma.
Related posts:


Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
