CHAPTER 61 Tricuspid and Pulmonary Valvular Disease
The tricuspid and pulmonary valves can fail as a result of disease states, which may lead to stenosis (Figs. 61-1 to 61-3), insufficiency (Figs. 61-4 to 61-6), or a combination of both (Figs. 61-7 to 61-9). Stenosis impedes forward flow, resulting in pressure overload, and insufficiency results in blood flowing backward, leading to volume overload. Tricuspid and pulmonary valvular disease may present in isolation or in conjunction. Clinical presentation, involvement of the cardiac chambers, severity of secondary chamber dysfunction, and impact on systemic and pulmonary vasculature and other viscera depend on which valves are involved, which type of valvular dysfunction predominates, the severity and duration of valvular dysfunction, and the degree of cardiac compensation. Pharmacologic, endovascular, and surgical management for diseased valves relies on accurate and comprehensive noninvasive diagnostic evaluation, using a combination of chest radiography, echocardiography, magnetic resonance imaging (MRI), magnetic resonance angiography (MRA), and computed tomography angiography (CTA). Invasive catheterization is no longer used to diagnose primarily tricuspid and pulmonary valvular disease and should be reserved for cases in which flow dynamics require direct assessment. Noninvasive modalities also form the basis for surveillance imaging.
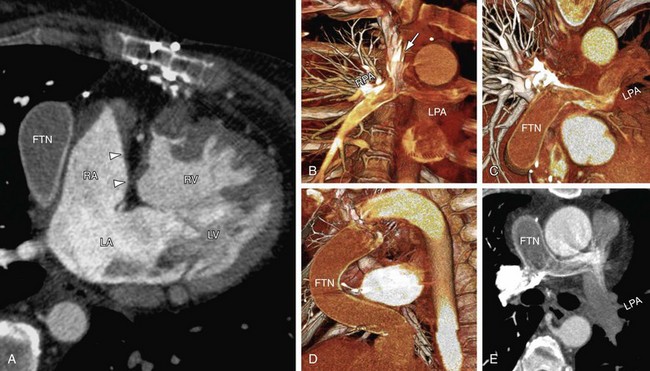
 FIGURE 61-1
FIGURE 61-1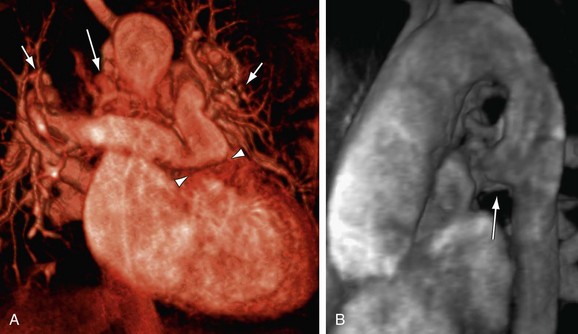
 FIGURE 61-2
FIGURE 61-2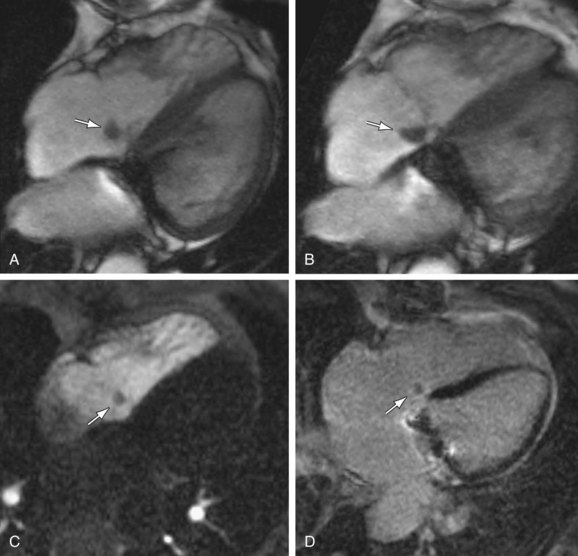
 FIGURE 61-3
FIGURE 61-3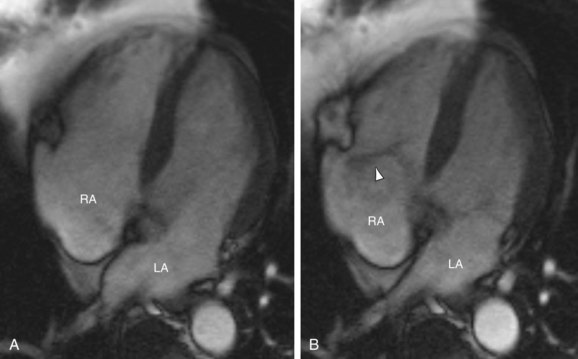
 FIGURE 61-4
FIGURE 61-4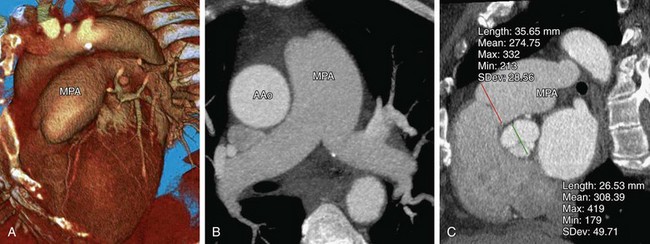
 FIGURE 61-5
FIGURE 61-5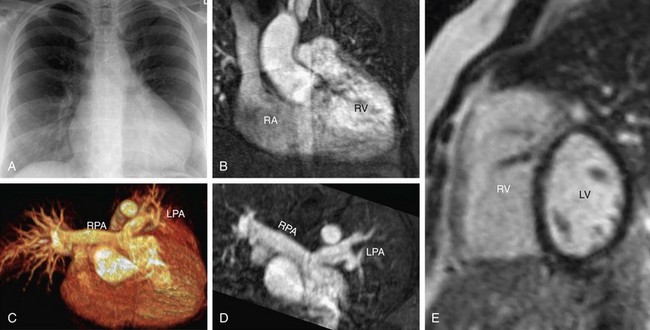
 FIGURE 61-6
FIGURE 61-6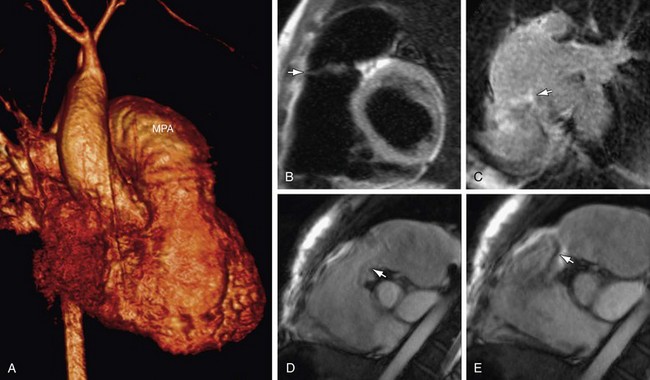
 FIGURE 61-7
FIGURE 61-7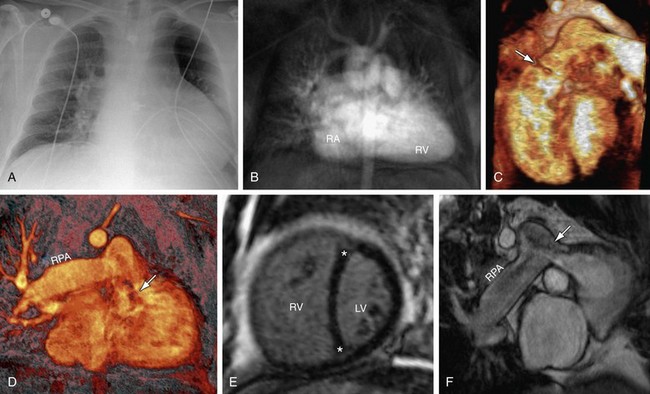
 FIGURE 61-8
FIGURE 61-8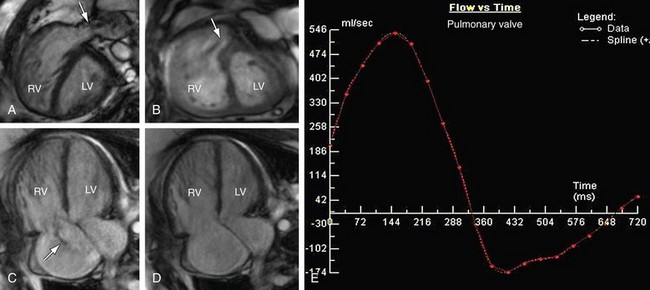
 FIGURE 61-9 Pulmonary stenosis and insufficiency with tricuspid insufficiency—functional analysis. Steady-state free precession short-axis and four-chamber projections from the patient shown in Figure 61-8 are shown in systole (A, C) and diastole (B, D). Turbulent signal (arrows) at the pulmonary valve corresponds to stenosis (A) and insufficiency (B). C, Turbulent signal (arrow) at the tricuspid valve corresponds to insufficiency. E, Quantitative analysis from phase contrast imaging yielded a pulmonary regurgitant fraction of approximately 25%.
FIGURE 61-9 Pulmonary stenosis and insufficiency with tricuspid insufficiency—functional analysis. Steady-state free precession short-axis and four-chamber projections from the patient shown in Figure 61-8 are shown in systole (A, C) and diastole (B, D). Turbulent signal (arrows) at the pulmonary valve corresponds to stenosis (A) and insufficiency (B). C, Turbulent signal (arrow) at the tricuspid valve corresponds to insufficiency. E, Quantitative analysis from phase contrast imaging yielded a pulmonary regurgitant fraction of approximately 25%.
TRICUSPID REGURGITATION
Anatomy and Normal Function of the Tricuspid Valve
The tricuspid valve is the right-sided atrioventricular valve, situated anterior and slightly apical in relation to the left sided mitral atrioventricular valve. It is aligned vertically, with anterior-left lateral angulation, in plane with the right ventricle and an orifice that is the largest of the four cardiac valves. The tricuspid valve is further distinguished from the mitral valve in that the mitral valve anteroseptal border is continuous with the aortic valve apparatus, whereas the tricuspid valve does not have any direct continuity to the pulmonary arterioventricular valve. Structurally, the tricuspid valve is composed of an annulus, three leaflets, and three commissures, which together with the right ventricle’s chordae tendinae, corresponding papillary muscles, and adjacent right atrium and right ventricle myocardium, form the tricuspid valve complex.1 The major function of the complex is to control leaflet aperture and closure. This process is governed by the pressure gradient between the right atrium and right ventricle, which in turn is regulated by preload, afterload, and myocardial contractility. Tricuspid valve opening occurs during ventricular diastole. It is closed during systole, preventing backflow. Physiologic tricuspid regurgitation occurs during systole; however, it may be found in structurally normal hearts of 17% to 65% of adults2–6 and 6.3% to 71% of pediatric patients,6,7 with most regurgitation being trivial to mild.
With regard to the components of the tricuspid valve complex, the annulus anchors the tricuspid valve to the right trigone of the cardiac fibrous skeleton, providing firm support for the entire complex. It is oval in shape and slightly larger than the mitral valve annulus, demarcating the boundaries of the tricuspid orifice.8 The annulus contracts during systole and reaches maximum size at end-systole.9 The mean major diastolic annulus diameter, area, and fractional shortening during three-dimensional echocardiography are reported to be 3.9 to 4.3 mm, 10 to 18.4 cm2, and 18.5% to 26%, respectively,1,8,10 whereas MRI values are reported to be 4.4 mm, 18.7 cm2, and 27%, respectively.8 Two-dimensional echocardiography underestimates annulus diameter and fractional shortening, with reported four-chamber values of 2.9 to 3.3 mm and 13.5% to 19%, respectively.
The three leaflets, labeled as anterior, posterior, and septal, are asymmetric in size, shape, and function.1 Each is attached to the annulus and separated and supported by the three commissures—anteroposterior, anteroseptal, and posteroseptal. Using three-dimensional echocardiography, Anwar and colleagues1 have reported the valve area to be 4.8 cm2 and each commissure to have an approximate width of 5 mm.
The anterior leaflet is the largest and most mobile, with a semicircular shape and an average width of 3.7cm.11 It is located anteriorly along the right ventricular free wall, extending from the anterolateral to inferolateral margin. The septal leaflet has a semioval shape, paralleling the interventricular septum, from anteroseptal margin to the posterior right ventricle wall. It is typically smaller than anterior leaflet, but is reported to have a width up to 3.6 cm.11 The septal leaflet is the least mobile of the three leaflets. The posterior leaflet extends along the posterior margin of the annulus from the inferolateral margin of the right ventricular free wall to the septum. It is variable in size and morphology, containing one or more (up to four) scallops, with an average width up to 2.8 cm.11
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


