Author and year
Number of patients
Hemorrhoid
Abcess
Perianal fistula
Recto-vaginal fistula
Anal fissure
Bargen 1929 [8]
693
26 (3.7%)
Jackman 1954 [7]
200
15 (7.5%)*
9 (4.5%)
Bockus et al. 1656 [6]
125
23 (18%)*
Edwards & Truelove 1964 [2]
624
129 (20.7%)
26 (4.2%)*
11 (3%)$
de Dombal et al. 1966 [1]
465
28 (6%)
25 (5.4%)
10 (3.6%)$
57 (12.3%)
Richard et al.
753
25 (3.3%)
13 (1.7%)
7 (0.9%)
12 (2.2%)
Zabana et al. 2011[4]
758
37 (5%)*
Anal stricture in UC has been described only as a complication of IPAA and is discussed below.
Perianal abscesses and/or fistulae in UC have been less well investigated than in CD. A few early studies reported a prevalence varying from 1.7% to 18%, with an average of 4.6%, which concurs with the findings reported in a recent study by Zabana et al. [4]. The latter study showed that these lesions occur in 5% of patients with UC, taking into account those with an initial diagnosis of the disease and in the 4% of patients who maintained the diagnosis (despite PAD) after a diagnostic reassessment. PAD develops more frequently in patients with active UC, in particular immunocompromised patients and those with increased requirements of steroid therapy [4,9]. It was also recently observed that UC complicated by perianal fistulae shows a greater and earlier requirement for steroids, immunomodulators, and biological therapy, mainly due to the PAD itself, compared with UC without PAD (Table 5.2).
Complex PAD carries relevant prognostic implications. It occurs mainly in patients in whom the initial diagnosis of UC will change to CD or indeterminate colitis and it is a significant risk factor for colectomy. Zabana et al. (2011) showed that in more than one-third of patients with UC and complex PAD the initial diagnosis changed, whereas this was not the case in any patient with simple PAD [4]. This study also showed that the prevalence of colectomy in UC patients with perianal fistulae and abscesses was nearly double that of patients without [4].
5.3 Ileo-Pouch-Anal-Anastomosis
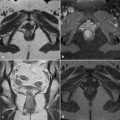
The main perianal complications of ileo-pouch-anal-anastomosis (IPAA) in patients with UC are strictures and fistulae. Symptomatic strictures may develop in up to 16% of patients [12–14]. Usually, the anastomotic stricture takes6–9 months to develop [15], appearing as web-like after a stapled IPAA or long and narrow after mucosectomy and a hand-sewn anastomosis. Strictures also may develop as a complication of cuff abscesses or of surgical techniques (e.g., following the use of a small circular stapler head, for mesenteric tension and partial anastomotic separation) [12].
Table 5.2
Disease course, major-disease related events and therapeutic approach in UC patients with and without perianal fistulae or abscesses (PAD) (modified from [4])