Chapter 12 Ultrasound as a Complement to Electrodiagnostic Studies
As the technology continues to improve and the literature in this field develops, the role of ultrasound in the electrodiagnostic evaluation will continue to evolve. The goal of this chapter is to review the current indications for ultrasound in regards to localization of nerve and muscle, to highlight the additional information ultrasound can provide in neuromuscular disease diagnosed electrophysiologically, and to touch on future research and directions for this imaging modality with respect to electrodiagnosis.
The Role of Ultrasound in Nerve Conduction Studies
Ultrasound can be used during nerve conduction studies to better localize the nerve in question at the site of stimulation or recording.1,2 The accuracy of near-nerve needle stimulation or recording is increased when nerves and surrounding structures are imaged and needles are placed under ultrasound guidance. Ultrasound-guided needle placement is a relatively easy technical skill to develop. Formal training courses are available with hands-on demonstration sessions, and the technique can be refined using fresh frozen cadavers or gel phantoms with enclosed targets for simulation of image-guided needle placement (Box 12.1). Once this skill is acquired, it facilitates the use of ultrasound as a complement to electrodiagnosis by enhancing the accuracy and safety of the invasive aspects of nerve conduction studies and needle EMG.
Box 12.1 Examples of Diagnostic and Interventional Ultrasound Educational Resources
American Association of Neuromuscular & Electrodiagnostic Medicine (AANEM): http://www.aanem.org/
American Institute of Ultrasound Medicine (AIUM): www.aium.org
European League Against Rheumatism (EULAR): www.eular.org
European Society of Skeletal Radiology (ESSR): www.essr.org
University of Michigan Ultrasound: www.med.umich.edu/rad/muscskel/mskus
Musculoskeletal Ultrasound Society (MUSOC): http://tdirad1.googlepages.com
Wake Forest University Center for Medical Ultrasound: http://www.wfubmc.edu/ultrasound/
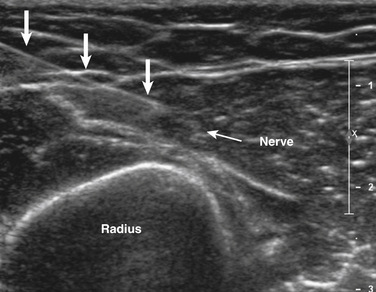
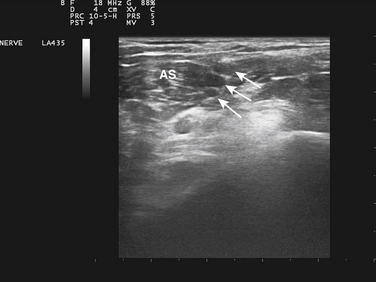
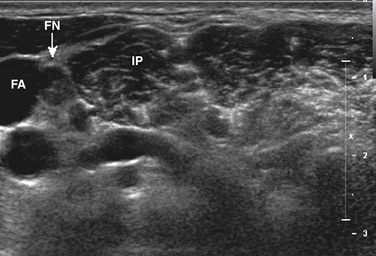
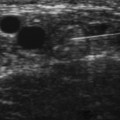
Ultrasound-guided needle placement can be very helpful in certain situations in the EMG laboratory. When apparent conduction block on a motor nerve conduction study is encountered but it is not clear whether technical factors such as submaximal stimulation may be contributing, a monopolar needle can be placed adjacent to the nerve, under ultrasound guidance, to allow for supramaximal stimulation (at much lower levels of current than required with surface stimulation). There are many potential applications for this, usually in nerves that are deeper and more difficult to stimulate with surface electrodes. Examples include the radial nerve at the spiral groove or elbow (Fig. 12.1), the sciatic nerve in the thigh, the tibial nerve at the knee, the femoral nerve in the proximal thigh, or even the brachial plexus or exiting cervical roots (Fig. 12.2).3 Femoral nerve stimulation may be indicated in cases of diabetic lumbosacral radiculoplexus neuropathy (diabetic amyotrophy) and select cases of Lambert-Eaton myasthenic syndrome, in which case repetitive stimulation before and after isometric exercise is necessary. In such cases, the neurovascular bundle is easily visualized with ultrasound and the needle can be placed directly adjacent to the nerve, allowing for less current, better patient comfort, and a technically superior response (Fig. 12.3). Such procedures can be also be more safely performed in anticoagulated patients, because the needle can be placed under direct ultrasound guidance, with visualization of nearby vascular structures facilitated by the use of color Doppler. The availability of ultrasound in this setting also allows for monitoring for hematoma formation after the needle is removed.
Ultrasound can also facilitate nerve conduction studies in challenging cases in which anatomy is altered or usual landmarks are not palpable as a result of body habitus or dysmorphism. In such cases, the nerve of interest can be localized ultrasonographically prior to proceeding with standard surface stimulation, for example, after ulnar nerve transposition surgery in which the altered position of the nerve can be mapped out in the antecubital fossa and inching studies performed along the actual course of the nerve.
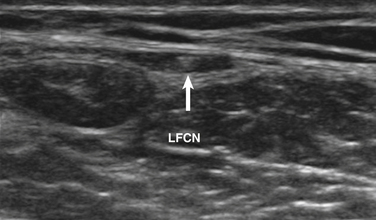
Ultrasound-guided nerve conduction techniques have been described to allow more accurate and reliable evaluation of nerves that previously had been difficult to study for technical or anatomic reasons. Examples include the lateral femoral cutaneous nerve in the proximal thigh and the saphenous nerve in the calf. Bailey and associates reported on a cohort of 50 normal subjects, including many with body mass indices in the obese range, in which the lateral femoral cutaneous nerve was localized with ultrasound, approximately 11 cm distal to the stimulation site at the inguinal crease (Fig. 12.4). The G1 electrode was placed directly over the nerve, and responses were elicited in 49 of 50 patients, with an average amplitude of 9.3 μV and side-to-side variability of 34%.4 Similarly, the saphenous nerve can be easily identified with ultrasound in the proximal calf and followed distally, to allow for placement of recording or stimulating electrodes directly over the nerve.5 If no response is obtained on standard conduction studies and there is a question as to whether technical factors may be contributing, it is simple to examine the limb with ultrasound and identify the nerve of interest, to ensure setup is optimal. In critical cases placing a needle next to the nerve for either stimulating or recording can be performed when necessary.
Imaging of Nerve
Ultrasound imaging of nerve is rapidly emerging as a useful diagnostic technique. In cases of entrapment neuropathy, electrodiagnosis helps to determine the presence and severity of entrapment, and to distinguish demyelination from axonal loss, but no information regarding the underlying cause can be elicited. Ultrasound can identify underlying space-occupying or compressive lesions such as lipoma, fibroma, hemangioma, hematoma, amyloid, synovitis, tenosynovitis, ganglion cyst, intraneural ganglion, pseudoaneurysm, anomalous muscle, and primary nerve tumors including neurofibromas, schwannomas, malignant nerve sheath tumors, and pericytomas.6–8 Typical sites of entrapment that can be evaluated with ultrasound are listed in Table 12.1.
Table 12.1 Common Sites of Entrapment that Can Be Evaluated with Ultrasound
| Nerve | Site of Entrapment |
|---|---|
| Suprascapular | Spinoglenoid notch, supraspinous notch |
| Axillary | Quadrilateral space |
| Radial | Spiral groove |
| Posterior interosseous | Supinator |
| Superficial radial | Wrist |
| Ulnar | Groove, cubital tunnel, wrist |
| Anterior interosseous | Mid-forearm |
| Median | Wrist |
| Sciatic | Thigh, posterior hip∗ |
| Peroneal | Fibular head |
| Superficial peroneal | Ankle, distal leg |
| Tibial | Ankle |
∗ The sciatic nerve can be difficult to visualize in the buttock/posterior hip region without the use of a curvilinear probe, particularly in obese patients.
Padua and colleagues used ultrasound imaging in a series of 77 cases presenting to the EMG laboratory with various mononeuropathies, including peroneal neuropathy at the fibular head, ulnar neuropathy at the elbow, and atypical median neuropathy at the wrist. In 26% of cases, an underlying cause for the neuropathy was identified on ultrasound, which led to an alteration in the management of those cases.8 Visser found intraneural ganglion cysts on ultrasound in 18% of patients with electrophysiologic evidence of common peroneal neuropathy at the fibular head.9 Similarly, in cases of suprascapular neuropathy, ultrasound of the posterior shoulder may identify a spinoglenoid cyst.10 In a series of 77 patients (96 wrists) with clinical and electrophysiologic evidence of carpal tunnel syndrome, without typical risk factors such as rheumatoid arthritis, diabetes, or pregnancy, 17% had evidence of underlying flexor tenosynovitis on ultrasound, which has implications with regard to management in comparison with cases of idiopathic carpal tunnel syndrome.7 Nakamichi and Tachibana showed that in patients presenting with unilateral carpal tunnel syndrome, 35% had an underlying structural abnormality, which altered the management in those cases.11 Anatomic variants, such as a bifid median nerve or persistent median artery, are easily identified on ultrasound and can have surgical implications, particularly with use of an endoscopic surgical technique, arguing for routine preoperative ultrasonography.
Ultrasound imaging is also useful in detecting complete nerve transection, which can be particularly helpful acutely, when electrodiagnostic studies cannot differentiate between conduction block and axonal injury.12 Neuromas can be easily identified on ultrasound. In addition, sonopalpation (direct pressure from the transducer applied over the area of interest) can be used to determine if a neuroma is symptomatic.13 Dynamic imaging is also useful in the diagnosis of various nerve disorders. For example, one can confirm the presence of a subluxing ulnar nerve, but more importantly, evaluate for a snapping head of the medial triceps, an entity that commonly accompanies a symptomatic subluxing ulnar nerve, and if unrecognized, can lead to a poor surgical outcome.14–15
When diagnosing nerve entrapment per se, as opposed to the underlying cause of the entrapment, there is a need for more studies evaluating both normal controls, diseased controls, and those with the entrapment of interest to delineate more accurately normal cross-sectional areas, the most appropriate site for measurement, the utility of patient-derived control measurements,16,17 and the effects of various body metrics on the normal values. Normal values for a number of nerves have been published.18 In particular, a number of studies have focused on median neuropathy at the wrist and ulnar neuropathy at the elbow with considerable overlap demonstrated between normal controls and those with the disease.7,14,18–22
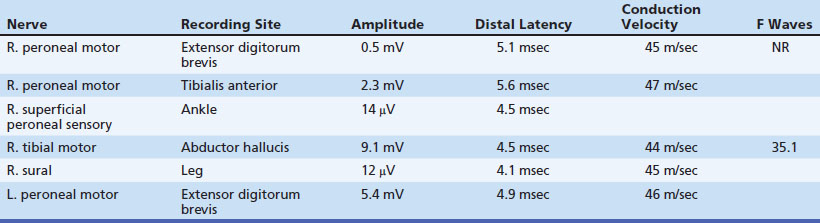
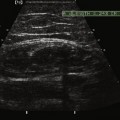
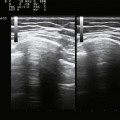
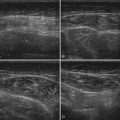
Clinical Application—Case 1
A 53-year-old man presented with a 6-month history of progressive pain during and after soccer games, progressing to pain and mild ankle weakness when hiking, that was unresponsive to antiinflammatory medication. On examination, the patient was noted to have mild to moderate weakness of ankle dorsiflexors and toe extensors on the affected side. Nerve conduction studies and needle examination demonstrated a common peroneal neuropathy, without focal conduction block or slowing (Tables 12.2 and 12.3). Ultrasound of the peroneal nerve showed a large intraneural ganglion cyst that was surgically decompressed (Fig. 12.5).


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


