Chapter 9 Ultrasound of Inflammatory Myopathies
B-Mode Ultrasound Dynamic Evaluation of Muscle Weakness in Myositis
Although the dimensions of normal muscle have been described in a few case series,1,2 the volumes obtained in practice are rather variable, and depend in part on the age and gender of the patient as well as the level of experience of the ultrasonographer.3,4 The reliability and validity of large muscle cross-sectional area measurements were demonstrated in a small study of six normal adults, when used by experienced examiners to monitor muscle thickness over time.5 When properly standardized with regard to location within the muscle, definition of muscle borders, and the angle of incidence (as outlined in Chapter 3), side-to-side comparison of a muscle in a particular patient and changes in muscle thickness can be detected serially over time.
The ability to distinguish between normal and weak muscle with ultrasound in the setting of muscle inflammation has been examined in one small study. Changes in rectus femoris muscle diameter (both horizontally and vertically) in the relaxed and contracted state were compared among nine patients with either “stable active or inactive myositis” (including six with idiopathic polymyositis, two with dermatomyositis, and one with inclusion body myositis, and nine normal patients).6 Horizontal diameter decreased and vertical diameter increased during isometric contraction in all patients. However, the average change in diameter was greater in control patients, and correlated with muscle force measured by dynamometry. These findings suggest that dynamic ultrasound may provide a quantitative adjunct to manual muscle testing in patients with myositis.
Standard B-Mode Ultrasound in Inflammatory Myopathy
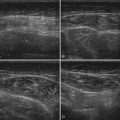
Several abnormal ultrasonographic morphologies have been described in the setting of inflammatory myopathy, including “edema-like,” “lipomatous,” and “chronic/atrophic” patterns. None of these patterns is disease specific, and a range of ultrasonographic findings has been described for all inflammatory myopathies.3,7,8
Muscle Edema
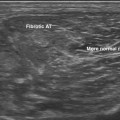
In contrast to the normal appearance of muscle (hypoechoic fascicles separated by the hyperechoic perimysial connective tissue), edematous muscle increases in size and echogenicity. This pattern can be observed transiently in the postexercise state,3 which underscores the importance of examining a patient at rest and not immediately after activation of the muscle of interest. This pattern is the least specific, as a multitude of posttraumatic, inflammatory, and infectious etiologies has been associated with muscle edema. Moreover, early infiltration by fat and fibrous tissue can have a similar ultrasonographic appearance, further reducing the diagnostic utility of increased muscle echogenicity.
Muscle Atrophy
Muscle atrophy can also be identified by ultrasound, and is characterized by increased echogenicity and reduced volume. In contrast to the edematous pattern, in which higher echogenicity is a result of increased water within the muscle, increased density of scattering interfaces and higher acoustic impedance is believed to be the cause in atrophy. Chronic infiltration by fat and fibrous tissue further increases muscle echogenicity. Thus, the combination of reduced muscle volume and increased echogenicity is characteristic of a long-standing process, consistent with either chronic inflammatory myopathy or denervation and disuse.9–11
Echogenicity
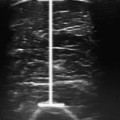
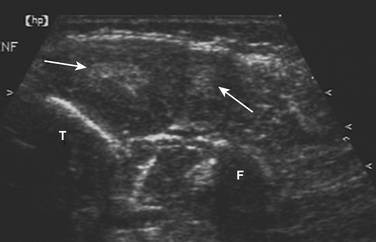
The degree of increased echogenicity, also referred to as echo intensity, can be estimated using either a subjective visual grading scale or quantitative methodology (Fig. 9.1). The most commonly used visual scale was developed by Heckmatt and associates initially for patients with muscular dystrophies.12,13 The Heckmatt score grades muscle echogenicity as grade I: normal echogenicity of muscle with a strong bone echo; grade II: increased muscle echogenicity but with a distinct bone echo; grade III: marked increase in muscle echogenicity, reducing the ability to identify the adjacent bone echo; and grade IV: very strong muscle echogenicity with complete loss of bone echo. Because of concerns regarding low interobserver agreement when using the visual rating scale,14 quantitative methods of measuring echogenicity using computer-assisted gray scale analysis have been developed. To facilitate reproducibility across different imaging platforms, ideal standards for machine configuration, calibration, probe positioning, and selection of the region of interest have been studied.15 As the reproducibility of quantitative gray scale analysis of muscle echogenicity is confirmed and more widespread experience is gained, it will likely come into more common clinical practice (see further discussion of qualitative and quantitative muscle echogenicity assessments in Chapters 3 and 10).
Doppler Ultrasound in Inflammatory Myopathies
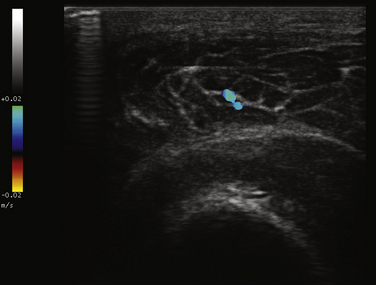
Power Doppler ultrasound provides a noninvasive means of estimating vascular volume and detecting soft tissue hyperemia.16 The technique is neither angle dependent nor subject to aliasing artifact, like conventional color Doppler imaging, which is also used for muscle imaging. However, power Doppler is not capable of measuring capillary flow, and will not differentiate between venous and arterial circulation.3 Doppler signal in muscle is also increased immediately after exercise because of a temporary increase in muscle vascularity, highlighting the importance of interpreting findings in recently exercised muscle with caution.17
One study designed to assess the utility of combining gray scale and Doppler techniques, examined 73 patients with inflammatory myopathies (including dermatomyositis [17], polymyositis [10], lupus-associated myositis [5], inclusion body myositis [3], focal myositis [1], and sarcoid myositis), and compared ultrasonographic and clinical findings (e.g., muscle power and function) with 6 control subjects. Significant differences between patients and controls were identified using both ultrasound techniques. Specifically, patients with shorter disease duration trended toward increased vascularity on Doppler measurements (Fig. 9.2), correlating with functional and inflammatory scores on clinical assessment. Abnormal findings on gray scale ultrasound (e.g., increased echogenicity and atrophy) were associated with longer disease duration and lower creatine kinase levels.18 The authors concluded that combining the two techniques may increase the ability to differentiate myositis from normal muscle, and help distinguish active from chronic muscle inflammation. A more recent case report highlighted similar findings in a patient with inflammatory myopathy, and resolution of the power Doppler abnormalities after treatment with steroids.19