Fig. 19.1
Lateral dose distribution of 140 MeV carbon ion beam and 70 MeV proton beam. Lateral falloff of the carbon ion beam is substantially sharper than proton beam
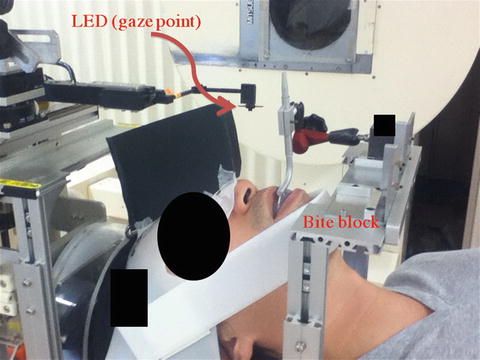
Fig. 19.2
Patient immobilization and eye fixation in the C-ion RT at the NIRS. A bite block is fixed to the bridge by strong magnet and gaze point can be set three-dimensionally with special head fixation devices
A set of 0.5-mm-thick CT images is obtained for the purpose of treatment planning using immobilization devices and a gazing light [11]. Titanium markers are sutured on the outer surface of the sclera for both treatment planning and field localization. Three-dimensional treatment planning had been performed using EYEPLAN software (NIRS, Chiba, Japan) until March 2005, and XiO-carbon combined with FocalPro (CMS Inc., St Louis, MO) has been used since April 2005. The contours of the target volumes and the organs at risk (e.g., lens, eyeball wall, optic disk) are drawn directly on the CT images. The gross tumor volume (GTV) is determined according to the CT images with reference to the ophthalmoscopy and MRI findings. The clinical target volume is almost the same as the GTV, with the exception that the clinical target volume has a 1.0–2.0-mm extra margin for possible tumor invasion into the sclera. Accordingly, the planning target volume (PTV) is automatically produced by the addition of an approximately ~1.0-mm margin to the CTV, but can be modified manually if necessary.
A compensation bolus and brass collimator are fabricated so that the PTV will be covered with greater than 95 % of the prescribed dose. In the beginning of the clinical trial, irradiation was delivered through a single anterior port; however, 2-port irradiation has been adopted for most patients since October 2005, because it seemed beneficial in reducing the risk of NVG. Indeed, the dose-volume histogram analysis using NIRS data indicated that the irradiated volume of the iris-ciliary body was related to the risk of NVG and that the V50 of the iris-ciliary body should be constrained to less than 0.1 mL [12, 13]. A typical dose distribution with 2-port irradiation is shown in Fig. 19.3.
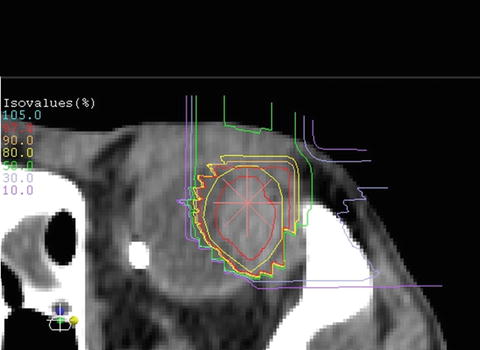
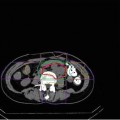
Fig. 19.3
Representative dose distribution of 2-port irradiation at the NIRS. The current prescribed dose is 70.0 GyE in 5 fractions for T3 tumor and 60.0 GyE in 5 fractions for T1/2 tumor
The prescribed total dose was varied from 60 GyE/5 to 85 GyE/5 fractions in the dose-escalation study and was fixed to 70.0 GyE/5 fractions for T3 tumors and 60.0 GyE/5 fractions for T1/2 tumors in the advanced treatment since April 2004.
19.3 Up-to-Date Outcomes of the C-ion RT at NIRS
As of February 2013, 127 patients with locally advanced or unfavorably located choroidal melanoma received CT-based C-ion RT at NIRS. Of these, 122 patients were followed up at least 6 months. The 5-year overall survival and eye retention rate were 80.8 and 93.1 %, respectively (Fig. 19.4). The local control rate of the treated tumors and the intraocular recurrence-free rate were 96.4 and 92.3 %, respectively (Fig. 19.5). These results are comparable to those of PRT (Table 19.1).
Fig. 19.4
Overall survival rate and eye retention rate of the patients treated with C-ion RT at the NIRS
Fig. 19.5
Local control rate of the treated tumor and intraocular recurrence-free rate after C-ion RT
Table 19.1
Treatment outcomes for particle radiotherapy of uveal melanoma
Institution | Particles | Number of patients | 5-year rate | ||
|---|---|---|---|---|---|
Local control (%) | Overall survival (%) | Eye retention (%) | |||
MGH | Proton | 1,006 | 96.3 |
||