, Lawrence A. Zumo2 and Valerie Sim3
(1)
Parkinson’s Clinic of Eastern Toronto, Toronto, ON, Canada
(2)
Silver Spring, Cheverly, MD, USA
(3)
Centre for Prions and Protein Folding Diseases, University of Alberta, Edmonton, AB, Canada
Abstract
In acute stroke, CT is the first modality of choice. A hyperacute ischemic stroke may appear normal or as blurring of the gray-white junction. At this stage, there is no enhancement with contrast. Acute ischemic stroke appears as an ill-defined hypodensity. There is usually no enhancement or only slight gyral enhancement at this stage. Subacute ischemic stroke appears a clear hypodensity with gyral enhancement. Acute and subacute haemorrhages appear hyperdense, whereas remote hemorrhages are hypodense. MRI diffusion weighting is helpful in demonstrating the restricted diffusion (cytotoxicity) of acute stroke and detecting smaller posterior fossa and brainstem infarcts. In this chapter, cases of ischemic and haemorrhagic stroke are presented.
Case 2.2 Acute Stroke: Sulcal Effacement
A 57 year-old right-handed male presented with a sudden onset of right hemiplegia and aphasia. He was imaged within 12 h of onset (Fig. 2.2).
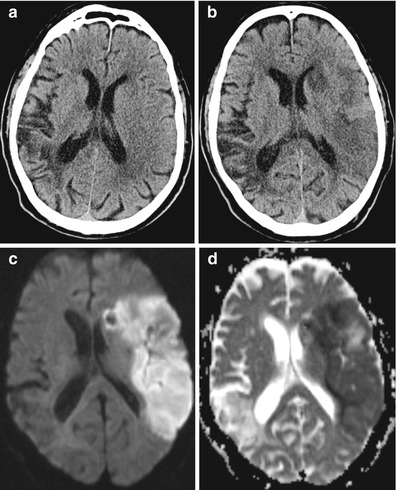
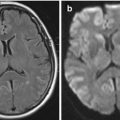
Figure 2.2
Axial CT scan of acute left middle cerebral artery stroke
Explanation and Diagnosis
Figure 2.2 shows a left frontoparietal sulcal effacement as well as a loss of grey-white junction. Clinically this man’s deficit did not resolve.
Case 2.1 Stroke Evolution
A 66 year-old left-handed female with a history of previous right parietal stroke presented with a 1 h history of sudden onset right hemiplegia and aphasia. CT and MRI imaging at 1 and 24 h was performed (Fig. 2.1).

Figure 2.1
Axial imaging of left middle cerebral artery stroke in evolution. (a) CT at 1 h; (b) CT at 24 h; (c) Diffusion weighted (DWI) MRI; (d) Apparent diffusion coefficient (ADC) MRI
Explanation and Diagnosis
The CT scan at 1 h (Fig. 2.1a) shows a hypodense old right parietal infarct and also early ischemia in the left middle cerebral artery territory: loss of grey-white junction in the anterior parietal lobe and loss of definition of the internal capsule. The areas of damage are better demonstrated as hypodensities on the CT scan at 24 h (Fig. 2.1b). MRI diffusion weighted and ADC images (Fig. 2.1c, d) also reveal the extent of acute ischemia. Clinically this woman’s deficit did not resolve.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


