KEY POINTS
Sonographic evaluation of the vertebral column and the spine is a requirement of almost all governing bodies.
Starting the 13th postmenstrual weeks it is possible to ascertain a normal spine as well as a number of its anomalies.
3D ultrasound is increasingly used and became instrumental in imaging the vertebral column in the three orthogonal planes using the X-ray or maximum mode rendering.
MRI may at times be necessary to complete the workup.
The assessment of the fetal vertebral column by transabdominal ultrasound (US) is an essential part of the second-trimester anatomical scan. The possibility of evaluating the spine at as early as 13 weeks of gestation by transvaginal high-resolution US has greatly improve its diagnostic capabilities and enabled the diagnosis of some of the common vertebral anomalies at this stage of pregnancy. Because not all spinal anomalies may be diagnosed during the late first or early second trimester, transabdominal US continues to be the “everyday” tool in the diagnosis of spinal and spinal cord malformations.1 One example of this is the tethered cord that may be visible, in some but not all the cases, from the the midsecond trimester as the terminal spinal cord becomes more clearly defined.
The introduction of volume US with minimum intensity projection, or radiograph mode, contributes to projecting and locating the exact level of the malformation.2 The additional value of this technology is still controversial, and the projection of a three-dimensional (3D) acquisition of the spine is not always reassuring, as it may miss small lesions in the lower spine.3
Magnetic resonance imaging (MRI) has been proposed as an additional tool in the diagnosis and counseling of patients with spinal cord anomalies, particularly regarding the evaluation of the spinal canal and its contents. So far this technology has not been widely used, but initial reports appear promising.4,5 In this chapter, the terms spine, spinal column, and vertebral column are used interchangeably.
The vertebrae develop during the sixth postmenstrual week of gestation, when chondrification centers appear for each mesenchymal vertebra. Each vertebral body has two primary ossification centers, one dorsal and one ventral. These centers fuse to form the centrum, which creates three primary ossification loci by the end of embryonic development; one develops in the vertebral body and the other two on each half of the vertebral arch.6 According to US studies, by 16 postmenstrual weeks, S1 and S2 ossification centers are almost all visualized in coronal planes, but S3 is present in only about half of these fetuses; the nucleus of S4 develops slightly later and is observed in all fetuses at 21 weeks.7 The posterior arch synchondrosis is not ossified in fetuses.
Closure of the neural tube seems to begin separately at several different levels. Progressive folding and closure of the neural structures and separation from ectoderm proceed both cranially and caudally from the point of initial closure, closing the neural tube in both directions. The most caudal end of the neural tube closes by 27 days of gestation. By 38 days, the lowest segment eventually becomes the most caudal portion of the conus medullaris, filum terminale, and ventriculus terminalis (focal dilation of the central canal in the conus medullaris).8
Because development and growth of the spinal cord are different from that of the vertebrae, the position of the conus medullaris in relation to the vertebral column is variable throughout pregnancy. On sagittal images, between 13 and 18 postmenstrual weeks, the conus medullaris is located below or at the level of L4 in all fetuses.9 Then it undergoes progressive ascent until term, when it is always located above the level of L2–L3 (Figure 17–1).10
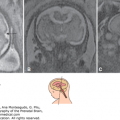
Figure 17–1.
Normal anatomy of the spine and the spinal cord in fetuses at 16 (A), 24 (B), and 28 (C) postmenstrual weeks in the sagittal section. Conus medullaris (large arrow); dura mater (small arrow). Note the progressive displacement of the position of the conus medullaris from L5 at 16 postmenstrual. Weeks to L2–L3 at 28 postmenstrual weeks.

Whenever possible, US should be performed, when the fetal spine is positioned close to the transducer. Manipulation of the fetal body to correctly position the fetus is usually relatively easy during the late first and early second trimesters. Closer to term it may be more difficult and in some cases impossible due to fetal size and the relatively lower amount of amniotic fluid. If possible, one should minimize the applied pressure to the transducer to leave amniotic fluid between the proximal uterine wall and the spine, to serve as an acoustic window. It is important to remember that the quality of US images is highly influenced by maternal habitus and fetal position, therefore in some cases optimal visualization of the fetal spine may be difficult or even impossible. Two-dimensional (2D) US evaluation of the spine is adequately covered in most US textbooks. We would like to discuss here the somewhat less employed but highly diagnostic yield of 3D US imaging the vertebrae.
The spine may be evaluated using three planes: sagittal, coronal, and axial (Figure 17–2). Usually only two of these planes may be obtained by 2D US. Sonographic evaluation of the fetal spine is possible due to the presence of the previously mentioned ossification centers within the fetal vertebrae.1,11

The sagittal planes enable visualization of the lateral ossification centers and each vertebral body. This is done by tilting the transducer from the midline (where the vertebral bodies are depicted) by about 15° to the right or left to reveal the lateral ossification centers. Fetal kyphosis may be identified in this plane. The skin, represented by an echogenic contour, should be meticulously evaluated to rule out the presence of skin-covered spinal dysraphism, which may be difficult or even impossible to detect, particularly before the third trimester. The curvature of the sacrum should be evaluated to include the normal anatomy of the rump to exclude sacral agenesis or sacrococcygeal teratoma. The spinal cord and meninges may be clearly visualized in these planes. Cord visualization is optimal in the fetus during the first and second trimesters due to partial bone mineralization and the small amount of soft tissue at the dorsum, creating a better sonolucent region than in the third trimester (see Figure 17–2).
The spinal cord is recognized as a hypoechoic tubular structure bordered by two echogenic lines, each line formed by the juxtaposed arachnoid and pia mater, with a hyperechoic central line representing the neural canal or the anterior median fissure.12 As pregnancy advances, the conus medullaris, which is the lower end of the spinal cord, ascends. A significant ascent of the conus medullaris is detected between 13 and 40 postmenstrual weeks from the level of L4 or below (between 13 and 18 weeks) to a level above L2 at term9 (see Figure 17–1). The visualization of a low-reaching conus medullaris during pregnancy should raise the suspicion of tethering.
The filum terminale, a delicate strand of fibrous tissue, appears as an echogenic midline string extending caudally from the conus medullaris through the coccyx.12 Abnormal thickening of the filum terminale has been reported in postnatal cases of tethered cord.13
The coronal planes display paired parallel ossification centers of the spine and help in the evaluation of the degree of scoliosis.1 Visualization of vertebral asymmetry raises the suspicion of hemivertebra (Figure 17–3).
Figure 17–3.
Hemivertebra with scoliosis. (A) At 14 postmenstrual weeks, the hemivertebra (black arrow) is clearly demonstrated in the coronal plane. (B) At 23 postmenstrual weeks, fusion of a normal vertebra and a hemivertebra is depicted as a large ossification center (white arrow) causing compression of the anterior and posterior borders of the cord (arrowhead).

The axial planes are produced by a dynamic shift starting either at the level of the head or from the sacrum cephalad and on the way demonstrate three ossification centers for each vertebra (see Figure 17–3). This plane is commonly used to exclude spinal defects and evaluate the overlying soft tissues.14 Chapter 5 contains additional, mostly 3D volume scans, with orthogonal displays and 3D renderings of the vertebral column.
Hemivertebra is a relatively common congenital anomaly of the spine in which only one-half of the vertebral body develops. The reported incidence of hemivertebra is 0.5 to 1.0 per 1000 births,15 with a male/female ratio of 0.31 for multiple vertebral anomalies and 0.68 for solitary vertebral anomalies.16 In this malformation, a portion of the vertebra does not develop, producing a wedge-shaped vertebra. Depending on which ossification center fails to develop, the hemivertebra may be lateral or dorsal.17 The main prenatal sonographic feature of hemivertebra is disruption of the normal spine alignment that leads to congenital scoliosis. When the suspicion of hemivertebra is raised, US is usually accurate in predicting the level and type of it. Usually the coronal plane allows the diagnosis by the display of the wedge-shaped hemivertebra and scoliosis (see Figure 17–3). By using the 3D multiplanar display with the volume acquisition in the midsagittal plane, the malformation may be projected forward, allowing observation of the exact level of the hemivertebra (Figure 17–4).

The diagnosis of isolated hemivertebra usually has a favorable outcome,18,19,20 but hemivertebra is frequently associated with other congenital anomalies, and a meticulous anatomical scan should follow its diagnosis. The whole spine, ribs, pelvis, and limbs should be scanned, as hemivertebra may be part of syndromes involving other skeletal anomalies.21 Extraskeletal anomalies, particularly cardiac and genitourinary tract anomalies, have been reported. They may be part of genetic syndromes, including Jarcho-Levin, Klippel-Feil, and VATER association (vertebral defects, imperforate anus, tracheoesophageal fistula, and radial and renal dysplasia).22
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


