39 Vocal cord paralysis is usually diagnosed clinically. However, it can be an incidental finding on neck computed tomography (CT) as 35% of patients with unilateral vocal cord paralysis may be asymptomatic and may have a normal voice. Imaging is often performed to find the cause of the paralysis; however, a radiographic cause is not demonstrated in at least half of all patients. The finding of atrophy/paralysis of the pharyngeal constrictor muscles with resultant dilatation of the ipsilateral pharyngeal wall has been described to differentiate a central vagal paralysis from a peripheral paralysis. In addition, the cricothyroid muscle is innervated by the superior laryngeal nerve, which arises from the proximal vagus nerve. If atrophy of this muscle is identified, then a proximal or central vagal lesion/neuropathy is present. It is important to recognize the findings of vocal cord paralysis and not to confuse any of the findings, such as thickening of the aryepiglottic fold or fullness of the paralyzed vocal fold, with other causes such as neoplasm. Over 90% of laryngeal and hypopharyngeal tumors are squamous cell carcinoma. Squamous cell carcinoma can involve any or all portions of the larynx (i.e., subglottic, glottic, supraglottic). CT and magnetic resonance imaging (MRI) are insensitive to superficial mucosal tumors without a significant exophytic component or submucosal extension. Two to five percent of laryngeal tumors will be non-squamous cell in etiology and several inflammatory and granulomatous processes can also involve the larynx.
Vocal Cord Lesions and Paralysis
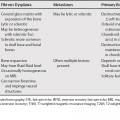
Vocal Cord Paralysis
Laryngeal Neoplasm
Findings Suggestive of Vocal Cord Paralysis
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


