How to Image the Wrist and Hand
See the wrist and hand protocols at the end of the chapter.
- •
Coils and patient position: Some type of surface coil is an absolute requirement for proper wrist imaging. Many different coils may be used, including dedicated wrist coils. Generally, the smaller the coil, the better the images of the wrist. If the patient is not too large, the wrist may be imaged with the patient supine and the arm alongside the body. For a larger patient, it may be impossible to image in this position; we usually have larger patients prone with the arm over the head and the elbow flexed. This position can become rapidly tiring and painful. The technologist must be aware of how to position and pad the patient properly at pressure points to ensure the patient’s comfort and prevent motion during the study. Padding under the shoulder and elbow is particularly useful. The best way to understand what is uncomfortable about an examination is to have it done to yourself.
- •
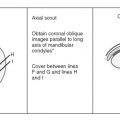
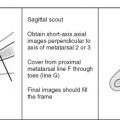
Image orientation ( Box 12-1 ): We image the wrist in three anatomic orthogonal planes, based on an axial scout view obtained through the proximal carpal row; this allows for acquiring true anatomic coronal, axial, and sagittal images. Many radiologists do not obtain sagittal images in the wrist, and this may be considered an optional sequence. We prefer to have sagittal images because they provide an additional look at the osseous structures and their alignment, which may not be evaluated as well in the other imaging planes.
BOX 12-1
Wrist Structures to Evaluate in Different Planes
Coronal
- •
Osseous structures
- •
Scapholunate ligament
- •
Lunotriquetral ligament
- •
Triangular fibrocartilage
- •
Dorsal and volar radioulnar ligaments
- •
Extrinsic ligaments of the carpus
- •
Ulnar collateral ligament of thumb
Axial
- •
Tendons
- •
Median nerve
- •
Ulnar nerve
- •
Carpal tunnel
- •
Guyon’s canal (ulnar tunnel)
- •
Distal radioulnar joint
Sagittal
- •
Carpal alignment
- •
Pisotriquetral synovial cyst
- •
- •
Pulse sequences and regions of interest: Pulse sequences are a combination of T1 and some type of T2 images. Gradient echo images are particularly excellent for ligament evaluation. Three-dimensional volume acquisition using gradient echo images allows for very thin (1-2 mm) slices, which are necessary for identifying the ligaments well. Two-dimensional gradient echo images that have a section thickness less than 3 mm also work well and can take less time to acquire. Protocols should be optimized for clinical indications, such as “routine” (pain), mass/infection, gamekeeper’s thumb, and trauma (screening for fractures only). We do dedicated imaging of only the wrist, unless there is a clinical reason given for imaging any portion of the hand as well. The field of view for a wrist examination is approximately ±10 cm (depending on patient size), and this allows the distal radius and ulna, carpal bones, and bases of the metacarpal bones to be included. An MRI examination of the hand includes the wrist, metacarpals, and most (or all) of the fingers, using the same pulse sequences and planes of imaging as for the wrist, but the field of view is enlarged to ±14 cm to include the additional anatomy. We also perform dedicated examinations of the fingers, in which case a 6- to 8-cm field of view is used. It is important to know the clinical indications to optimize the field of view. The coronal plane of imaging shows the small ligaments of the wrist best, and it is essential to have thin slices in this plane. For evaluation of ligaments, the slice thickness should be 1 to 2 mm. A slice thickness of 3 mm can be used in the other imaging planes and for evaluation of masses, fractures, and other abnormalities aside from ligaments.
- •
Contrast: Intravenous contrast administration is used to evaluate a mass to differentiate a cystic from a solid lesion as well as to evaluate for infection to appreciate abscess formation better. Because of concern of partial tears of intrinsic ligaments and triangular fibrocartilage complex (TFCC), MR arthrography can be performed with contrast injection in the radiocarpal joint space (intrinsic ligaments) or distal radioulnar joint space.
Normal and Abnormal
LIGAMENTS
The ligaments of the wrist are divided into intrinsic and extrinsic ligaments. The intrinsic carpal ligaments connect carpal bones to one another and limit their motion. The extrinsic ligaments connect the bones of the forearm to the bones of the wrist, allowing stability of the wrist with the distal forearm.
Intrinsic Ligaments ( Box 12-2 )
Normal Scapholunate and Lunotriquetral Ligaments.
The scapholunate ligament and the lunotriquetral ligament are the two intrinsic carpal ligaments of greatest clinical significance; disruption of these ligaments may cause instability and pain. Both of these ligaments can be evaluated best on gradient echo coronal images using thin sections. These ligaments are horseshoe-shaped, bandlike, or triangle-shaped structures on the proximal aspects of the carpal bones to which they attach ( Fig. 12-1 ).
Scapholunate and Lunotriquetral, Most Important
- •
Maintain alignment among carpal bones
- •
Triangular, horseshoe, or bandlike shapes on proximal aspects of bone, attaching to bone or cartilage
- •
Low signal with areas of intermediate signal traversing (normal)
- •
Scapholunate abnormalities
- •
Stretched or torn
- •
MRI—90% accurate
Discontinuity, absence, irregularity, thinning with high signal on T2 traversing ligament defect
Increased intercarpal space, sometimes
Elongation (stretching) of undisrupted ligament
- •
- •
Scapholunate ligament abnormalities may lead to
- •
Rotatory subluxation of scaphoid
- •
Dorsal intercalated segmental instability
- •
Scapholunate advanced collapse wrist
- •
- •
Lunotriquetral ligament tears may lead to
- •
Volar intercalated segmental instability
- •
- •
Associated with triangular fibrocartilage complex tears

The scapholunate ligament has volar, middle, and dorsal portions ( Fig. 12-2 ). Studies have shown that only the volar and, especially, the dorsal portions are important for wrist stability. The volar portion is looser so that it can accommodate the various articulating curvatures of the scaphoid and lunate. Perforations (or communicating defects) in the middle portion are common and do not seem to relate to symptoms when they are an isolated finding.

The volar portion of the scapholunate ligament is trapezoidal in configuration, with intermediate signal intensity on gradient echo images. The middle portion of the scapholunate ligament is triangular in shape, with lower signal intensity than the volar component, and both portions are routinely heterogeneous in signal intensity. The dorsal portion, the most important for carpal stability, is a low signal intensity, homogeneous band. Generally, the volar portion of the scapholunate ligament attaches to cortical bone, whereas the middle and dorsal portions attach to hyaline cartilage or a combination of cartilage and cortical bone. The reason for the higher signal intensity of the volar and middle portions of the scapholunate ligament compared with the dorsal portion is related to the lower density of collagen fibers and the higher proportion of loose connective tissue and vascular tissue in these regions.
The lunotriquetral ligament is smaller and more taut than the scapholunate ligament, but has a similar shape and frequently displays a heterogeneous low signal intensity on coronal gradient echo images. The lunotriquetral ligament may attach to hyaline articular cartilage or cortical bone. Its stronger and thicker volar component blends with the triangular fibrocartilage (TFC).
Intermediate signal intensity may partially or completely traverse the substance of the lunotriquetral ligament and scapholunate ligament in asymptomatic individuals ( Fig. 12-3 ). It should be considered an abnormal finding (torn ligament) only if this signal intensity is as high in signal as that of fluid on whatever type of T2 sequence is being used. Similarly, high signal intensity between articular cartilage and the ligament should indicate an avulsed ligament only if the signal intensity is as bright as fluid.

Abnormal Scapholunate and Lunotriquetral Ligaments.
Scapholunate instability is the most common carpal instability. Clinically, patients complain of pain and weakness on the dorsal radial aspect of the wrist. Abnormalities on MRI that indicate a scapholunate ligament abnormality are listed:
- 1.
Discontinuity of the ligament, with or without an increased space between the scaphoid and lunate bones
- 2.
Complete absence of the scapholunate ligament
- 3.
Distorted morphology with fraying, thinning, and irregularity
- 4.
Elongated ligament with an increased intercarpal space ( Fig. 12-4 )

Figure 12-4
Scapholunate ligament abnormality. A , Coronal fat-suppressed T2W image shows fluid signal between the scaphoid and lunate ( arrow ). Scapholunate distance is wide. B , Fast T2 with fat saturation coronal image of the wrist (different patient than in A ). There is distortion of the morphology of the scapholunate ligament, which is frayed and with a vertical high signal tear through it ( arrows ). C , Gradient echo coronal image of the wrist (different patient than in A and B ). The space between the scaphoid and lunate bones is increased, and the ligament ( arrow ) is stretched, although it remains intact. This was the result of inflammation associated with rheumatoid arthritis. Multiple bone erosions, subchondral cysts, and a triangular fibrocartilage tear also are present.
The accuracy of MRI has been reported as 90% compared with arthrography and 95% compared with surgery (arthroscopy and arthrotomy).
Scapholunate instability occurs when the scapholunate ligament is completely torn or stretched, allowing the scaphoid and lunate bones to dissociate. The scaphoid tilts in a volar direction (rotatory subluxation), whereas the lunate tilts in a dorsal direction (dorsal intercalated segmental instability). The relationship of the osseous structures can be detected on sagittal MRIs ( Fig. 12-5 ). Rotatory subluxation is the most common instability pattern in the wrist. The dorsal intercalated segmental instability pattern of carpal instability also can occur with an unstable fracture of the scaphoid, even though the scapholunate ligament is intact. Partial tears more commonly affect the weaker volar ligamentous attachment.

Scapholunate ligament disruption and chronic rotatory instability of the scaphoid also may lead to the capitate migrating proximally and may cause scapholunate advanced collapse (SLAC) wrist. The SLAC wrist consists of scapholunate ligament disruption, degenerative changes between the scaphoid and the distal radius, and proximal migration of the capitate between the scaphoid and lunate bones ( Fig. 12-6 ).

Disruption of the lunotriquetral ligament is not as easy to diagnose as disruption of the scapholunate ligament because of its smaller size. Similar abnormalities to those seen in an abnormal scapholunate ligament are present in an abnormal lunotriquetral ligament ( Fig. 12-7 ). Tears of the lunotriquetral ligament are the second most common cause of carpal instability and result in the lunate tilting in a volar direction (volar intercalated segmental instability) secondary to the disruption of the triquetral attachment. There is a strong association between tears of the TFC and lunotriquetral ligament tears. The alignment of the carpal bones on sagittal images depends on wrist position. The lunate tends to volar flex and dorsiflex relative to the radius when the wrist is placed in radial and ulnar deviation. Proper positioning of the hand and wrist in the magnet is important to prevent this pitfall. Normally, the distal radius, lunate, and capitate all align colinearly, or nearly so, just as they do on a lateral wrist radiograph.

Extrinsic Ligaments
Volar and Dorsal Ligaments.
The extrinsic carpal ligaments can be seen best on gradient echo coronal images; they are seen in cross section on sagittal images ( Fig. 12-8 ). These ligaments course between the carpal bones and the radius on the volar and the dorsal sides of the wrist. The extrinsic ligaments run obliquely and are best imaged on oblique sagittal images. Because imaging usually is not done in this plane, it generally requires several adjacent coronal images to see an entire ligament. The volar ligaments are stronger and thicker than the dorsal ligaments and are major stabilizers of wrist motion. Extrinsic ligaments are thickenings of the joint capsule and are intracapsular and extrasynovial. Extrinsic ligaments appear as striated fascicular structures with alternating bands of low and intermediate signal intensity on coronal MRIs.

The most important volar ligaments are the radioscaphocapitate and radiolunotriquetral ligaments. The radioscaphocapitate ligament originates on the volar surface of the radial styloid process and courses obliquely across the waist of the scaphoid without attaching to it (it acts as a seatbelt to maintain the position of the scaphoid), to insert on the center of the capitate. The radiolunotriquetral ligament is the largest ligament of the wrist. It arises adjacent to (on the ulnar side of) the radioscaphocapitate ligament on the radial styloid. It runs obliquely to attach to the volar surfaces of the lunate and triquetrum.
The dorsal extrinsic ligaments of the wrist run obliquely between the distal radius and to each of the carpal bones of the proximal carpal row (radioscaphoid, radiolunate, and radiotriquetral ligaments). There are other small extrinsic carpal ligaments that are not discussed here.
The good news about all of these extrinsic ligaments is that no one knows with certainty what importance they have clinically. The MRI appearance of normal extrinsic ligaments has been extensively described, but the ability of MRI to detect abnormalities is unknown. The only value in radiologists knowing about them is so that they do not cause confusion during interpretation of MRIs of the wrist. We spend little to no time analyzing these ligaments.
TRIANGULAR FIBROCARTILAGE COMPLEX ( Box 12-3 )
The TFCC is the primary stabilizer of the distal radioulnar joint and is composed of several soft tissue structures on the ulnar side of the wrist: the TFC, volar and dorsal radioulnar ligaments, meniscus homologue, ulnar collateral ligament, and the sheath of the extensor carpi ulnaris tendon ( Fig. 12-9 ).
Components
- •
Triangular fibrocartilage
- •
Radioulnar ligaments (dorsal and volar)
- •
Extensor carpi ulnaris tendon sheath
- •
Ulnar collateral ligament
- •
Meniscus homologue
Function
- •
Absorbs axial loading forces (20% pass through ulnar side of wrist)
- •
Stabilizes ulnar side of wrist and distal radioulnar joint
Abnormalities
- •
Triangular fibrocartilage
- •
Partial-thickness or full-thickness tears, detachment, degeneration
- •
High signal through surface on T2 = tear
- •
- •
Radioulnar ligaments
- •
High signal through these structures indicates a tear
- •
Tear leads to instability of distal radioulnar joint
- •
- •
Extensor carpi ulnaris sheath
- •
Tenosynovitis commonly affects this tendon
- •
High signal surrounding tendon on axial T2 images
- •
Disruption of the sheath leads to medial subluxation of extensor carpi ulnaris from its groove in ulna
- •

The functions of the structures that compose the TFCC include cushioning forces across the ulnar side of the wrist during axial loading and stabilizing the ulnar side of the wrist and the distal radioulnar joint. With neutral ulnar variance, about 80% of axial loading forces pass through the radial side of the wrist. The ulna absorbs about 20% of the axial loading forces through the TFCC.
Triangular Fibrocartilage
Normal Triangular Fibrocartilage.
The TFC is a fibrocartilaginous biconcave disk with an asymmetric bow-tie shape, similar to the temporomandibular joint disk ( Fig. 12-10 ). The TFC is positioned in the ulnocarpal space with attachments on the medial side to the ulnar styloid process by two thin bands of TFC tissue. At its radial attachment, there is hyaline cartilage interposed between the TFC and the radius that must not be confused with a detached or torn TFC. The TFC attaches directly to the cartilage, which is the articular surface of the distal radioulnar joint. The thickness of the TFC is inversely proportional to the degree of ulnar variance. In other words, the TFC is thinner in patients with positive ulnar variance, which may predispose it to tear, and thicker in patients with negative ulnar variance. The TFC is depicted best on coronal MRIs. It may be diffusely low signal intensity regardless of pulse sequence, or have intermediate signal intensity in its substance from asymptomatic myxoid degeneration.

Abnormal Triangular Fibrocartilage.
Any structure of the TFCC can be abnormal, but the TFC is the main component to show abnormalities. Clinically, patients complain of ulnar-sided wrist pain and tenderness. An audible click with pain may be elicited by rotation of the forearm. On MRI, the TFC can be evaluated similarly to the meniscus in the knee. High signal intensity within the substance of the TFC has no clinical significance, whereas high signal intensity extending through either the proximal or the distal surface of the TFC indicates a tear ( Fig. 12-11 ). TFC tears may be partial or full thickness, extending partially or completely through the substance of the TFC. Partial tears are noted more frequently at the proximal articulating surface with the distal radioulnar joint. Fluid in the distal radioulnar joint was previously believed to be a secondary sign of a TFC tear, but a small amount of fluid may be present in this joint in most individuals.

The location of a tear has therapeutic implications because of the vascular supply of the TFC. The peripheral 20% of the TFC on the ulnar margin is well vascularized, and tears may heal with nonoperative therapy if properly immobilized or with primary repair. The remainder of the TFC is essentially avascular, and perforations or tears in the central and radial portions of the TFC usually are débrided. Many individuals have high signal intensity within the substance of the TFC and perforations, but have no symptoms. The intrasubstance signal is probably from myxoid degeneration. The asymptomatic perforations are probably degenerative in nature because most traumatic tears are symptomatic. As with all imaging, the presence of abnormal findings does not ensure that symptoms are a consequence of the abnormalities, and correlation of the MRI and clinical findings is mandatory in planning proper management of patients. The TFC may be traumatically detached from its ulnar attachment and may become interposed between the radius and ulna, preventing proper reduction of the distal radioulnar joint ( Fig. 12-12 ).

Traumatic tears of the TFC often are associated with injuries of adjacent structures, such as the extensor carpi ulnaris tendon sheath and lunotriquetral ligament, which can be shown readily by MRI. MRI is very accurate for diagnosing TFC tears; compared with arthrography and surgery, it has an accuracy rate of 95%. Tears in the central and radial portions are best shown, whereas tears near the ulnar attachment are less accurately diagnosed because synovitis or synovial proliferation in the prestyloid recess may mimic a tear.
Radioulnar Ligaments
Normal Radioulnar Ligaments.
The volar and dorsal radioulnar ligaments are broad, striated bands that originate on the volar and dorsal cortex of the sigmoid notch of the distal radius. The ligaments pass on the volar and dorsal surfaces of the TFC and blend with it. The radioulnar ligaments attach to the ulnar styloid process medially, and to the distal radius laterally. The dorsal and volar radioulnar ligaments can be distinguished from the TFC proper because they tend to have flat superior and inferior margins, rather than being biconcave, and they attach directly to bone, rather than to cartilage on the radius ( Fig. 12-13 ). These structures are low signal intensity on all pulse sequences and are best depicted on coronal images.

Abnormal Radioulnar Ligaments.
Disruption of the volar or dorsal radioulnar ligaments is associated with instability of the distal radioulnar joint. Disrupted ligaments can be seen on MRI, and subluxation or dislocation of the distal radioulnar joint can be shown easily on axial MRIs ( Fig. 12-14 ). Distal radioulnar joint instability is diagnosed when the ulna does not articulate properly with the sigmoid notch of the distal radius and is displaced in either a dorsal or volar direction from this notch.

Meniscus Homologue
The meniscus homologue can be thought of as a thickening of the ulnar side of the joint capsule that is inconsistently present. It is located just distal to the prestyloid recess and attaches to the triquetrum. If present, it is shown on coronal MRIs as a low signal intensity, triangle-shaped structure ( Fig. 12-15 ). The prestyloid recess is a triangle-shaped space bordered by the meniscus homologue distally, the TFCC attachments to the ulnar styloid process proximally, and the central TFC disk radially. The prestyloid recess normally contains fluid.

Extensor Carpi Ulnaris Sheath
Normal Extensor Carpi Ulnaris.
The extensor carpi ulnaris tendon and its sheath, which is a component of the TFCC, can be seen on coronal MRIs, but is best depicted in the axial plane, as is the case with many other tendons ( Fig. 12-16 ). The tendon sheath is not evident on MRI, unless there is fluid in it. The extensor carpi ulnaris tendon is located in the groove on the dorsum of the ulna in neutral and pronation positioning of the wrist, whereas subluxation can be seen if imaged in supination.

Abnormal Extensor Carpi Ulnaris Sheath.
Traumatic disruption of the extensor carpi ulnaris tendon sheath can result in subluxation or dislocation of the extensor carpi ulnaris tendon at the level of the distal ulna, out of its normal groove, in a medial direction. Associated tenosynovitis is common. Subluxation and tenosynovitis are best shown on axial images ( Fig. 12-17 ).

Ulnar Collateral Ligament (Wrist)
The ulnar collateral ligament of the wrist is an additional support structure making up the TFCC that may be seen on coronal MRIs (see Fig. 12-10A ). It represents a thickening of the wrist joint capsule and provides little mechanical strength. The ulnar collateral ligament extends from the ulnar styloid process to the triquetrum. A similar structure exists on the lateral side, the radial collateral ligament, which extends from the radial styloid process to the scaphoid.
ULNAR COLLATERAL LIGAMENT OF THE THUMB
Normal Ulnar Collateral Ligament of the Thumb
The normal ulnar collateral ligament of the thumb is a taut structure that attaches to the base of the proximal phalanx of the thumb and to the distal end of the first metacarpal. It stabilizes the ulnar aspect of the first metacarpophalangeal joint. On MRI, the ligament is a low signal intensity band that spans the first metacarpophalangeal joint, located deep to a similar, vertically oriented low signal intensity band, which is the adductor aponeurosis ( Fig. 12-18 ). Highresolution imaging with a small field of view oriented to anteroposterior of the view of the thumb (coronal to the thumb) is necessary to see this structure properly.

Gamekeeper’s Thumb
An abduction injury to the first metacarpophalangeal joint may cause an avulsion fracture at the site of attachment of the ulnar collateral ligament to the base of the proximal phalanx of the thumb (one third of cases), or it may injure only the ulnar collateral ligament without radiographic evidence of an osseous abnormality (two thirds of cases). MRI of a tear of the ulnar collateral ligament simply shows the thin, low signal intensity ligament avulsed from the base of the thumb or discontinuity of the ligament with hemorrhage and edema surrounding the torn ends of the ligament (see Fig. 12-18 ). The ligament remains deep to the linear adductor aponeurosis. The edema and hemorrhage are high signal intensity on T2W images. Gradient echo images are excellent for showing the ligament well.
When the ulnar collateral ligament is retracted proximally and displaced superficial to the adductor aponeurosis, it is referred to as a Stener lesion . Stener lesions occur in about one third of all gamekeeper’s thumbs. The interposition of the adductor aponeurosis between the torn ligament and the bone prevents healing, which may lead to chronic laxity, loss of grip, and degenerative joint disease. Treatment of a Stener lesion in the first 3 weeks after injury has a better outcome than more delayed treatment and may warrant MRI for diagnosis because physical examination is inaccurate for this lesion.
A Stener lesion has been described as having the appearance of a yoyo on a string on MRI. The yoyo is created by the balled-up and retracted ulnar collateral ligament, and the string of the yoyo is the adductor aponeurosis (see Fig. 12-18C ).
TENDONS
Normal Anatomy
Tendons in the wrist are best depicted in the axial plane. Most of the flexor tendons (nine tendons) pass through the carpal tunnel on the volar aspect of the wrist. It is unnecessary to know the names of individual flexor tendons.
The extensor tendons are located on the dorsum of the wrist and are important to know. The extensor tendons are stabilized on the dorsum of the wrist by an extensor retinaculum. Fascial septations form six dorsal compartments that contain the extensor tendons ( Fig. 12-19 ).