Wrist Ultrasound
KEY FACTS
GENERAL CONSIDERATIONS
TECHNIQUE
 Patient seated across examiner with wrist resting prone on adjustable table
Patient seated across examiner with wrist resting prone on adjustable table
 ± small pad under hypothenar eminence to align wrist and carpus in more horizontal position
± small pad under hypothenar eminence to align wrist and carpus in more horizontal position
 Wrist in lateral position ± ulnar deviation to scan scaphoid/1st extensor compartment
Wrist in lateral position ± ulnar deviation to scan scaphoid/1st extensor compartment
 Wrist in lateral position ± radial deviation to scan ulnocarpal articulation/6th extensor compartment
Wrist in lateral position ± radial deviation to scan ulnocarpal articulation/6th extensor compartment

Clinical photograph shows the scan position for the dorsal wrist. A small pad  can be placed under the ulnar aspect of the wrist to align the dorsal wrist more horizontally.
can be placed under the ulnar aspect of the wrist to align the dorsal wrist more horizontally.

Longitudinal US shows the distal radius  , lunate
, lunate  , and capitate
, and capitate  all aligned. The soft tissue interposed between the carpus and extensor digitorum tendon
all aligned. The soft tissue interposed between the carpus and extensor digitorum tendon  is composed of joint synovium, extrinsic ligaments, and loose areolar tissue. These individual elements cannot be discerned.
is composed of joint synovium, extrinsic ligaments, and loose areolar tissue. These individual elements cannot be discerned.

Longitudinal US shows the distal radius  , scaphoid
, scaphoid  , and trapezoid
, and trapezoid  all aligned. The bony irregularity
all aligned. The bony irregularity  on the dorsum of the scaphoid is normal. Such irregularity of normal bone contour does somewhat limit US assessment of a carpal fracture.
on the dorsum of the scaphoid is normal. Such irregularity of normal bone contour does somewhat limit US assessment of a carpal fracture.

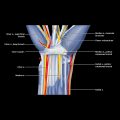
Axial intermediate-weighted MR of the wrist at the level of the distal radioulnar joint shows the 1st  , 2nd
, 2nd  , 3rd
, 3rd  , 4th
, 4th  , 5th
, 5th  , and 6th
, and 6th  extensor compartments.
extensor compartments.
GENERAL CONSIDERATIONS
Clinical Indications for Wrist US
TECHNIQUE: DORSAL WRIST
Patient Position
Specifically Examine
 Composed of 3 distinct compartments
Composed of 3 distinct compartments
 All 3 joints are best viewed using dorsal approach as joints are more superficial
All 3 joints are best viewed using dorsal approach as joints are more superficial
 Scan transversely over distal radius/ulna to view DRUJ
Scan transversely over distal radius/ulna to view DRUJ
 Rotate transducer into longitudinal plane to view radiocarpal/ulnocarpal and midcarpal joints
Rotate transducer into longitudinal plane to view radiocarpal/ulnocarpal and midcarpal joints
 Note joint distension, hypoechoic/hyperechoic synovial proliferation, and joint fluid deep to echogenic capsule
Note joint distension, hypoechoic/hyperechoic synovial proliferation, and joint fluid deep to echogenic capsule
 Color Doppler imaging and especially, to lesser degree, compression can help differentiate fluid from synovitis
Color Doppler imaging and especially, to lesser degree, compression can help differentiate fluid from synovitis
 Place ulnar border of wrist on table ± resting on pad used to help ulnar deviate wrist
Place ulnar border of wrist on table ± resting on pad used to help ulnar deviate wrist
 Note larger APL and smaller EPB
Note larger APL and smaller EPB
 Both tendons rest on shallow groove in radial styloid covered by echogenic extensor retinaculum (< 0.5 mm thick)
Both tendons rest on shallow groove in radial styloid covered by echogenic extensor retinaculum (< 0.5 mm thick)
 1/3 of wrists have septum (90% complete,10% partial) between APL and EPB
1/3 of wrists have septum (90% complete,10% partial) between APL and EPB
 95% of APL tendons have multiple slips while < 5% of EPB tendons have > 1 slip
95% of APL tendons have multiple slips while < 5% of EPB tendons have > 1 slip
 Superficial radial nerve branches pass over ± under 1st extensor compartment from volar to dorsal wrist
Superficial radial nerve branches pass over ± under 1st extensor compartment from volar to dorsal wrist
 4th compartment contains 4 ED tendons (1 for each finger) and EIP tendon
4th compartment contains 4 ED tendons (1 for each finger) and EIP tendon
 4th compartment of extensor retinaculum is thickest
4th compartment of extensor retinaculum is thickest
 Passive finger movement can help identify tendons
Passive finger movement can help identify tendons
 5th extensor compartment is fibrous rather than fibroosseous and overlies DRUJ
5th extensor compartment is fibrous rather than fibroosseous and overlies DRUJ
 Visibility of small EDM can be improved by moving little finger; EDM typically joins ED tendon just proximal to metacarpophalangeal joint
Visibility of small EDM can be improved by moving little finger; EDM typically joins ED tendon just proximal to metacarpophalangeal joint
 Best examined with wrist fully pronated & ulna facing up
Best examined with wrist fully pronated & ulna facing up
 Observe ECU within groove on ulnar head covered by fibrous retinaculum (ECU subsheath)
Observe ECU within groove on ulnar head covered by fibrous retinaculum (ECU subsheath)
 For dynamic assessment of ECU, flex elbow with ulnar head facing examiner
For dynamic assessment of ECU, flex elbow with ulnar head facing examiner
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree