Diagnosis: Left ovarian torsion in a patient with polycystic ovarian syndrome (PCOS)
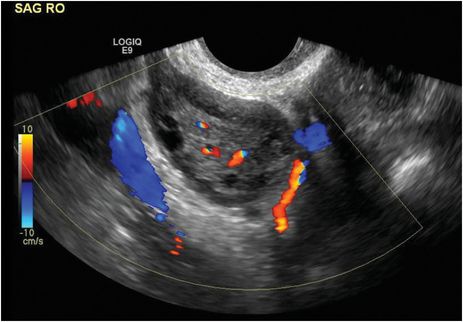
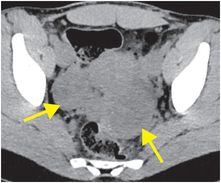
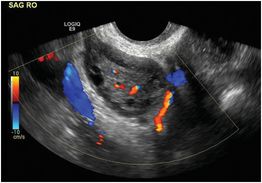
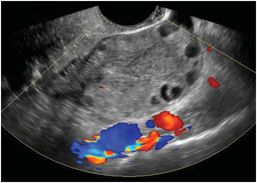
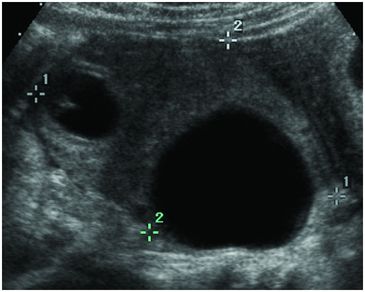
Axial noncontrast abdominal CT demonstrates enlargement of both ovaries (arrows) in this patient with a history of polycystic ovarian syndrome (PCOS). The left ovary is slightly larger than the right. Grayscale and color Doppler ultrasound images of each ovary (right ovary: middle image; left ovary: right image) in the same patient demonstrate enlarged ovaries with multiple small peripheral follicles (“string of pearls” sign). The left ovary appears enlarged and heterogeneously echogenic compared to the right, with absent blood flow.
Discussion
Ovarian torsion is most common in women of reproductive age, and 20% of cases occur during pregnancy.
Ovarian masses (acting as “lead points”) and other conditions that result in ovarian enlargement predispose to torsion. In cases without a lead point, ligamentous laxity or vascular tortuosity may be risk factors. The risk of ovarian torsion during the first trimester of pregnancy is increased due to the corpus luteum, which acts as a lead point.
Women undergoing fertility treatments are also at increased risk due to enlargement of numerous follicles, especially with concomitant ovarian hyperstimulation syndrome (OHSS).
Torsion of the normal ovary can occur in prepubescent females because of adnexal hypermobility, usually on the right side.
Ovarian torsion may have a nonspecific clinical presentation of pelvic pain, nausea, and vomiting. Symptoms may be intermittent.
There is symptomatic overlap with many mimickers, including appendicitis, gastroenteritis, pelvic inflammatory disease, ectopic pregnancy, and ruptured ovarian cyst.
Ultrasound is the most sensitive imaging modality for ovarian torsion, and, hence, the modality of choice in most scenarios where torsion is suspected.
As a general rule, ovarian torsion is extremely rare when the ovary is normal in size, echogenicity, and position. The most common imaging finding is asymmetric enlargement of one ovary due to venous congestion, with peripheralization of follicles.
A cystic or mass-like structure interposed between the uterus and bladder is highly suggestive of torsion.
Free pelvic fluid is present in up to two-thirds of cases.
Common CT and MR imaging features include fallopian tube thickening, smooth wall thickening of a cystic adnexal mass that appears twisted, ascites, uterine deviation to the side of the abnormal adnexa, and an adnexal mass rotated out of the pelvis to the contralateral side of midline.
Color and spectral Doppler analysis is neither sensitive nor specific, but is routinely performed.
Normal ovaries may have no detectable Doppler signal due to technical factors, while blood flow or even hyperemia may be seen in an ovary that is undergoing intermittent torsion with transient vascular obstruction.
The sonographic “twisted vascular pedicle” or “whirlpool” sign is highly suggestive of torsion. A twisted pedicle may only be visible with Doppler overlay. Absence of flow in the twisted pedicle, or flow in only the artery and not the vein may be seen in cases of torsion.
The most common treatment for ovarian torsion is laparoscopic surgery with manual detorsion and removal of any underlying mass that has acted as a lead point.
In patients who have experienced torsion, there is a 10% increased incidence of torsion in the contralateral adnexa at another point in time.
Clinical synopsis
Laparoscopy confirmed left ovarian torsion, and the left ovary was detorsed.
Self-assessment
|
|
|
|
|
Spectrum of ovarian torsion
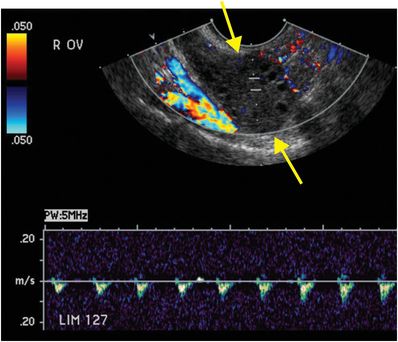
Right ovarian torsion with preserved arterial flow
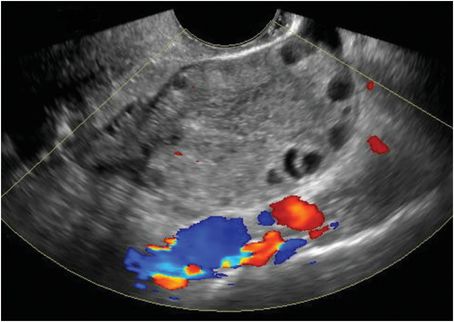
Color and spectral Doppler ultrasound in a patient with right-sided pelvic pain demonstrates asymmetric enlargement and hyperechogenicity of the right ovary (arrows). There is diminished arterial perfusion with absence of diastolic flow of the right ovary. In torsion, venous congestion leads to ovarian edema, which is generally followed by progressive arterial compromise.
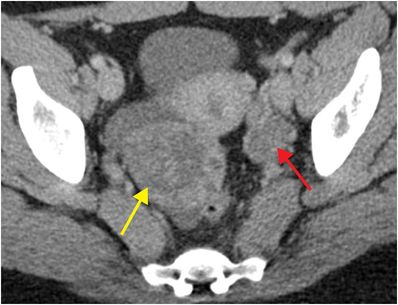
Right ovarian torsion with complete absence of flow
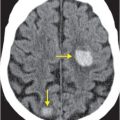
This 25-year-old female presented with acute right lower quadrant pain. Contrast-enhanced axial CT demonstrates a markedly enlarged, heterogeneous right ovary (yellow arrow) with surrounding fluid. The left ovary (red arrow) is normal in size. Color Doppler ultrasound demonstrates an enlarged, avascular, heterogeneously echogenic right ovary with small peripheral follicles. The diagnosis of ovarian torsion was confirmed intraoperatively.
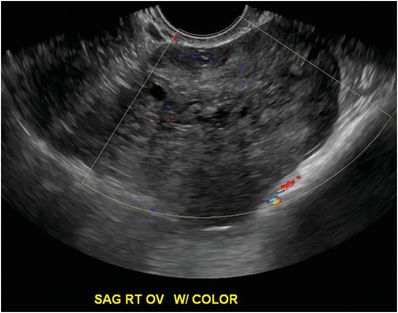
Torsion in a patient with ovarian hyperstimulation syndrome (OHSS)
This patient with a history of pharmacologic ovarian stimulation for treatment of infertility presented with pelvic pain. Grayscale transvaginal ultrasound image demonstrates an enlarged (9 cm) right ovary containing multiple hypoechoic cysts and intervening edematous stroma. OHSS is a serious complication of pharmacologic ovulation induction. Early in the course, there is mild ovarian enlargement with abdominal discomfort. Later, there is marked enlargement of the ovaries, with pelvic pain, abdominal distention, nausea, and vomiting. The typical sonographic finding is bilaterally enlarged ovaries with multiple large cysts that produce a “spoke wheel” appearance. Pregnant patients with OHSS have a greater risk of torsion (16%) than those who are not pregnant. Separation of the cystic elements by the markedly edematous stroma may indicate torsion of the hyperstimulated ovary.
Related posts:
 12 68-year-old man with left lower quadrant pain and hypotension
12 68-year-old man with left lower quadrant pain and hypotension
 72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
 35 37-year-old woman with a history of rheumatoid arthritis presenting with non-resolving bilateral effusions and chest pain
35 37-year-old woman with a history of rheumatoid arthritis presenting with non-resolving bilateral effusions and chest pain
 62 38-year-old male complaining of diffuse abdominal pain after a motor vehicle collision
62 38-year-old male complaining of diffuse abdominal pain after a motor vehicle collision
 51 90-year-old male with elevated blood pressure and change in mental status. No history of trauma
51 90-year-old male with elevated blood pressure and change in mental status. No history of trauma
 66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


