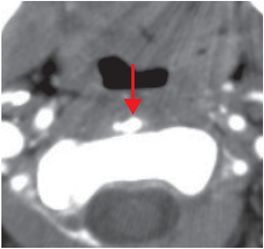
Diagnosis: Longus colli calcific tendinitis (acute calcific prevertebral tendinitis)
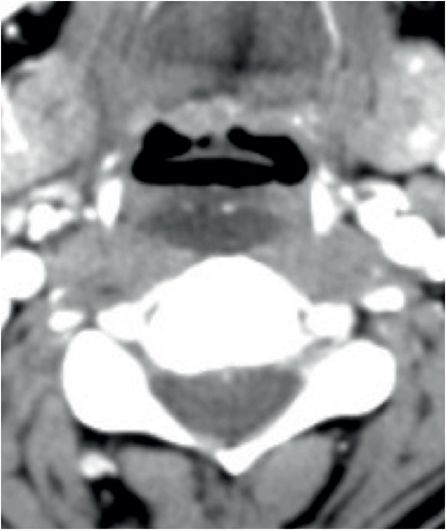
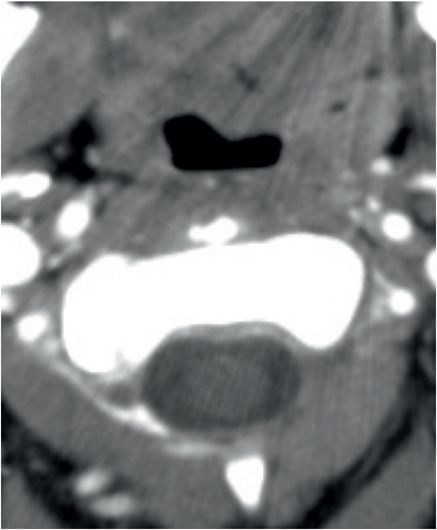
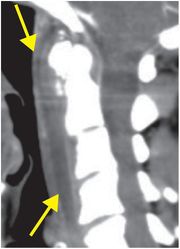
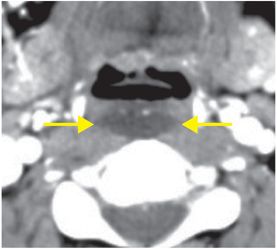
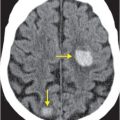
Sagittal (left image) and axial (middle and right images) contrast-enhanced CT images reveal a non-enhancing, hypodense prevertebral collection (yellow arrows) extending from C1 through C4–C5. Axial CT at the level of the dens shows prevertebral calcification (red arrow) in the location of the longus colli tendon. The fluid collection produces minimal mass effect.
Discussion
Overview and clinical presentation of calcific prevertebral tendinitis
Acute calcific prevertebral tendinitis is a benign, self-limited, acute inflammatory condition of the longus colli tendon. Like calcific tendinitis elsewhere in the body, it is characterized by intra-tendinous calcium hydroxyapatite deposition.
The typical presentation is acute onset of neck pain, sore throat, and dysphagia. Patients are usually in minimal distress and have, at most, low grade fever. Laboratory analysis may show mild leukocytosis and elevated erythrocyte sedimentation rate. Whereas retropharyngeal abscess is seen in children, immunosuppressed patients, and following penetrating trauma, longus colli tendinitis tends to affect healthy adults.
Imaging of calcific prevertebral tendinitis
Imaging findings include a prevertebral/retropharyngeal effusion that typically extends from C1 to C4–C5 or C5–C6. A calcium deposit at the C1–C2 level is seen on cross-sectional imaging.
Diffuse enhancement may occur; however, rim enhancement, a more typical feature of abscess, is absent. There are no associated suppurative lymph nodes or jugular venous thrombi.
Treatment and differential diagnosis
Treatment of calcific prevertebral tendinitis is non-operative, and includes NSAIDs and observation.
The differential diagnosis includes retropharyngeal abscess, jugular venous thrombophlebitis resulting in retropharyngeal edema or effusion, cellulitis, soft tissue mass (such as a suppurative lymph node), and foreign body. The most important distinction is between infected and non-infected collections, as management differs in these two entities.
Clinical synopsis
This 43-year-old woman was treated conservatively with NSAIDs and recovered uneventfully.
Self-assessment
|
|
|
|
Related posts:
 12 68-year-old man with left lower quadrant pain and hypotension
12 68-year-old man with left lower quadrant pain and hypotension
 72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
 35 37-year-old woman with a history of rheumatoid arthritis presenting with non-resolving bilateral effusions and chest pain
35 37-year-old woman with a history of rheumatoid arthritis presenting with non-resolving bilateral effusions and chest pain
 62 38-year-old male complaining of diffuse abdominal pain after a motor vehicle collision
62 38-year-old male complaining of diffuse abdominal pain after a motor vehicle collision
 51 90-year-old male with elevated blood pressure and change in mental status. No history of trauma
51 90-year-old male with elevated blood pressure and change in mental status. No history of trauma
 66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


