Fig. 30.1
(a) Pre-op anteroposterior radiograph; note reduced joint space in the left hip. (b) False profile view: arrow shows ossified labrum anteriorly
MRI
Labral tearing of the anterior and lateral portions of the labrum. Chondral thinning and fissuring; lateral center-edge angle is 23°; alpha angle is 76°; femoral retroversion is 4°. Moderate effusion with capsular scarring and extensive synovitis, debris, and possible loose bodies. A prominent osteophyte was observed around the cotyloid fossa (Fig. 30.2a, b).
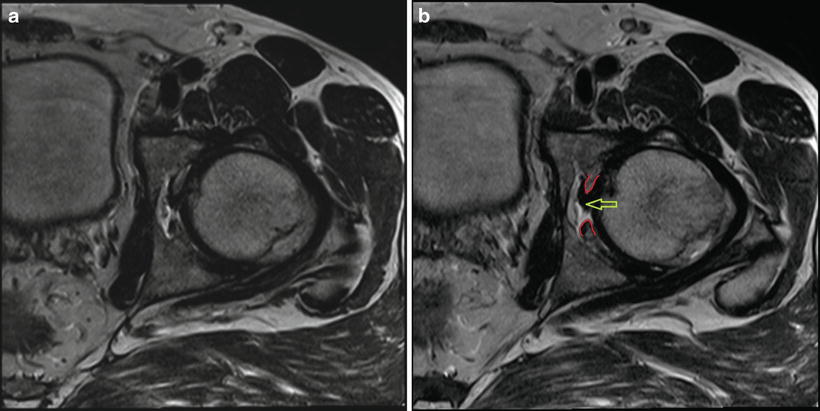
Fig. 30.2
(a, b) MRI of cotyloid fossa stenosis—axial view. Red lines: border of osteophytes causing the cotyloid fossa stenosis. Yellow arrow: ligamentum teres
Arthroscopy
The patient underwent a left hip arthroscopy, synovectomy, rim trimming, neck osteoplasty, removal of loose bodies, cartilage debridement, and chondroplasty,
An ossification of the acetabular labrum from 8:00 to 2:00 position was observed. This was removed with an osteotome and a burr. A labral reconstruction was performed with a 50 mm IT band graft and six suture anchors.
There was a grade 4 acetabular chondral defect of roughly 30 × 15 mm. Microfracture was used to treat this lesion (Fig. 30.3).

Fig. 30.3
Microfracture using an arthroscopic awl
With the hip in distraction, the cotyloid fossa was inspected, and osteophytes were removed from this area to allow the femoral head to be well seated within the acetabular cup and to release the ligamentum teres entrapment. To accomplish this, we utilized different instruments such as an osteotome, burr, chisel, and basket punch (Fig. 30.4a–e).
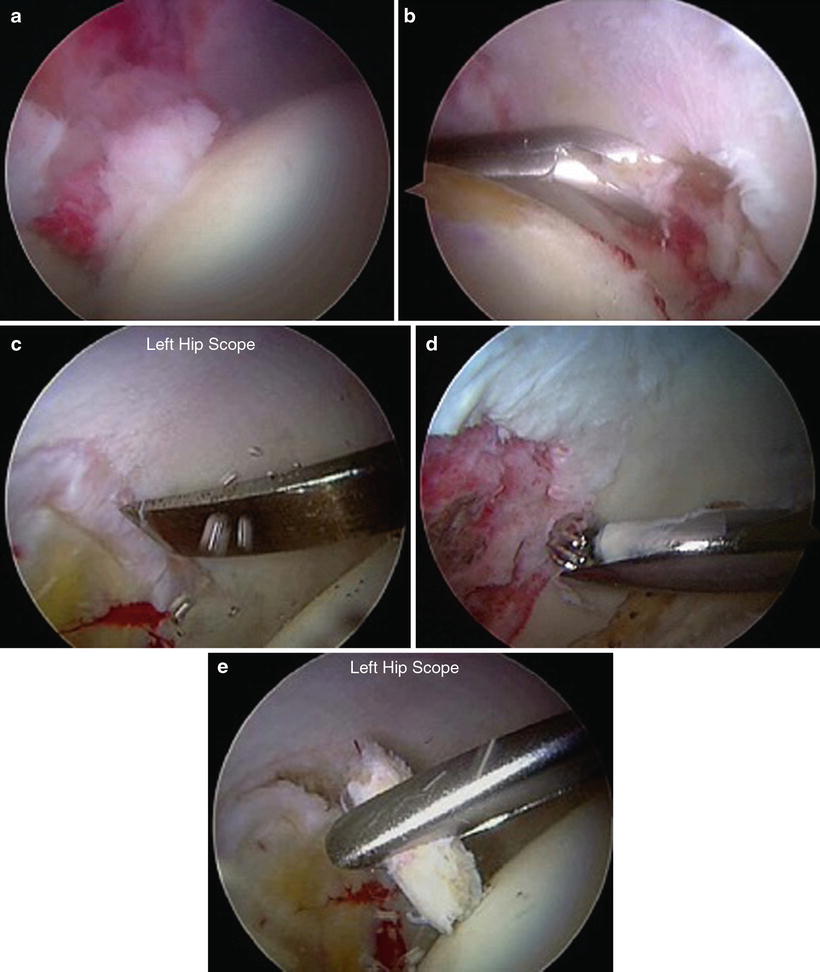
Fig. 30.4
(a) Fossa stenosis; ligamentum teres entrapment. (b) Osteophyte removal with a basket punch. (c) Chisel used for osteophyte removal. (d) Fossa stenosis decompression with burr. (e) Osteophyte removed with grasper
After this, we debrided the ligamentum teres with the RF device, removing the inflamed synovium around it so it would sit better inside the cotyloid fossa (Fig. 30.5).
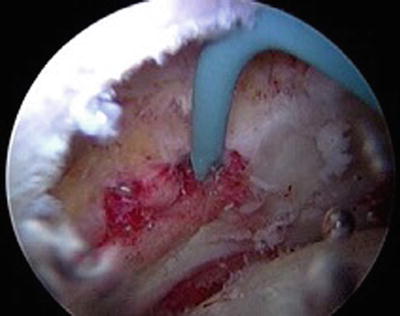
Fig. 30.5
LT debridement
After the cotyloid fossa stenosis and LT debridement, we observed a better congruence between the femoral head and the cotyloid fossa. Traction was released so a dynamic assessment could be performed, and the femoral head could glide freely inside the acetabulum with restoration of the fluid seal.
Discussion
This case reveals the multifactorial nature of hip dysfunction in the active patient with moderate osteoarthritis. The acetabular rim, sclerotic and with ossified labrum, was a component of lost joint motion. The large cam-style femoral osteophyte also contributed. The theoretical contribution of space-occupying degenerative acetabular fossa contents also appeared to contribute. Attention to the deep central hip compartment arthroscopically was guided by clinical suspicion and the MRI findings of synovitis, effusion, and acetabular fossa stenosis. Further study is required to advocate global acceptance of this type of debridement, but preliminary case-based evidence is promising.
Case 2: Ligamentum Teres Reconstruction
History
Female, 25 years old, softball coach. Patient had already undergone two prior right hip arthroscopies and two left hip arthroscopies.
The last left hip surgery (1 year before) included labral debridement, lysis of adhesions, chondroplasty, synovectomy, psoas lengthening, and a labral reconstruction using an IT band autograft.
The patient complains of left hip pain that continues to bother her daily. She has signs of hip instability. She complains of her left hip giving out multiple times a day, preventing her from performing daily activities. Sometimes she has the feeling that the hip “pops out.”
Past surgical history: positive for multiple surgeries on both hips, both shoulders, and left foot.
Exam
Normal strength of the muscles surrounding the hip joint, including hip flexors bilaterally. Normal sensation throughout lower extremities. Positive anterior impingement sign. Physical exam is consistent with generalized laxity. ROM: flexion 126°, abduction 45°, and adduction 30°. Grossly positive left hip manual distraction test.
Imaging
Radiographs
Joint space was preserved (>2 mm). Sourcil measuring 2–3 mm, anterior sourcil 3 mm. Tonnis angle is 5.5°. Lateral center-edge angle is 29°. Alpha angle is 43°. Sharp angle is 42°. See Fig. 30.6.

Fig. 30.6
AP pelvis before surgery
MRI
Labral reconstruction appears stable, without any gross separation identified. Diminutive ligamentum teres with signs of scarring and possible prior debridement. A complete LT tear could be present. See Fig. 30.7a, b.
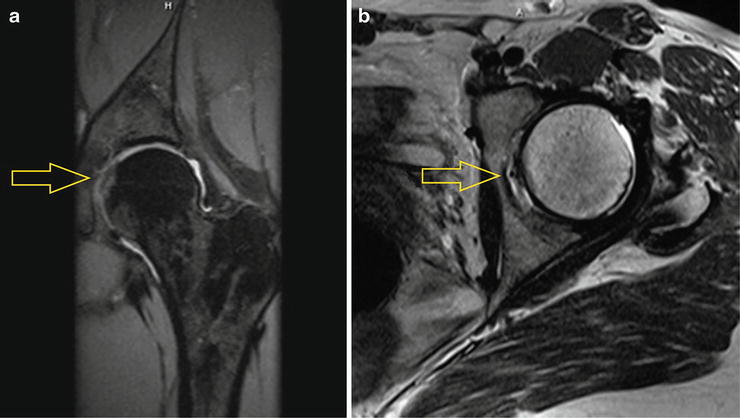
Fig. 30.7
(a, b) MRI pre-op: ligamentum teres is frayed and cannot be precisely outlined, which could be due to a complete tear
Arthroscopy
Before putting the leg into table traction, a physical exam was performed under anesthesia. The joint could be distracted with manual traction alone, confirming severe hip laxity (Fig. 30.8).
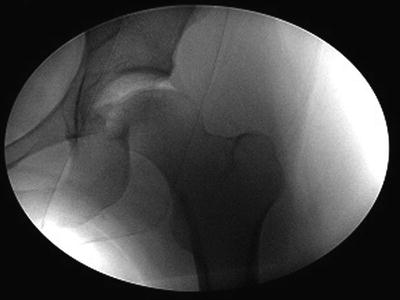
Fig. 30.8
Effortless manual distraction of the hip joint, under anesthesia
Initial arthroscopic inspection: significant synovitis throughout the joint, significant adhesions especially at the capsulolabral recess, and a visible ligamentum teres tear (Fig. 30.9).
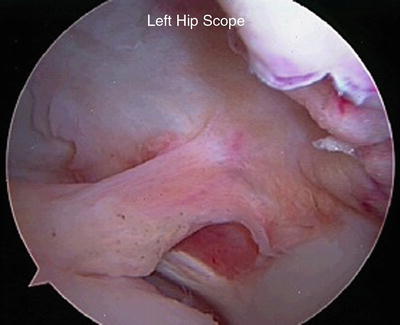
Fig. 30.9
Torn insufficient ligamentum teres
Synovectomy was done using a combination of the electrocautery wand, ablator, and shaver. Hemostasis was assured with the RF device.
We then removed the adhesions by using the RF ablator and shaver, clearing up the capsulolabral recess. The labral reconstruction was intact and the suction seal was restored once the adhesions were removed.
Ligamentum teres: the LT was torn and grossly insufficient. The scar tissue surrounding it was debrided.
To begin the LT reconstruction, the arthroscopic shaver and burr were used to debride the cotyloid fossa, partially removing the pulvinar fat, and to expose the footprint of the ligamentum teres.
Then, using the C-arm, a K-wire was inserted from the lateral cortex of the femur, in line with the femoral neck. The trajectory was 1 cm below the center of the neck, so the tip of the K-wire would exit at the femoral fovea. The correct position of the K-wire was confirmed at both lateral and AP views (Fig. 30.10).
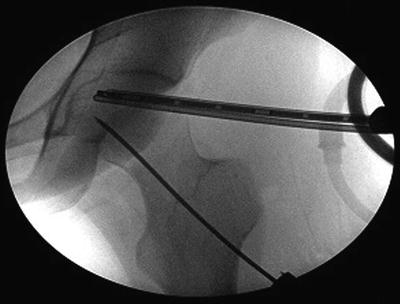
Fig. 30.10
K-wire is drilled into the femoral neck with c-arm and arthroscopic guidance
We then drilled a hole using a cannulated 6 mm reamer over this K-wire. This was then enlarged to 7 mm and finally to 8 mm. The tunnel went all the way to the femoral fovea, and a curette was placed inside the joint to protect the acetabular joint surface from damage by the reamer and the K-wire (Fig. 30.11a–c).
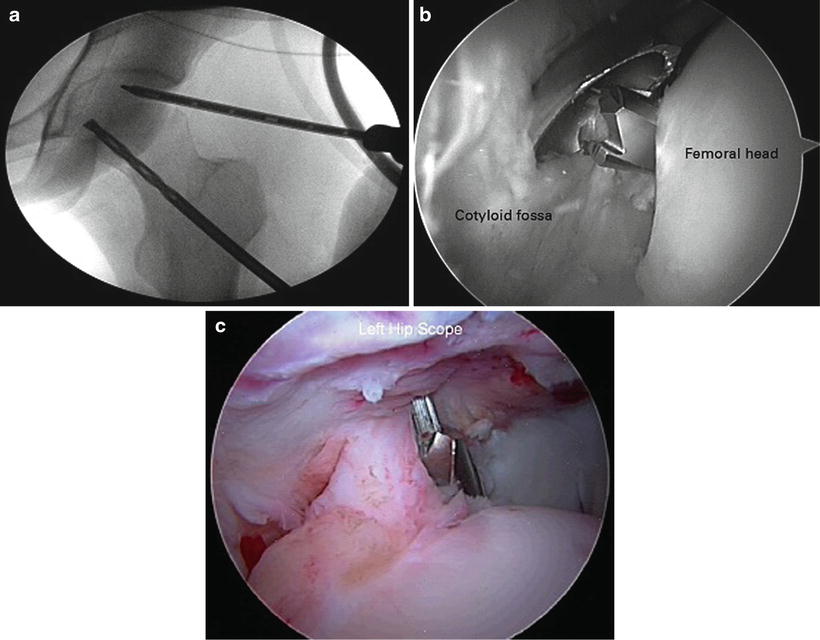
Fig. 30.11
(a) The 8 mm tunnel is made with a reamer. (b) A curette is used to protect the acetabular surface. (c) Drill bit exiting through the fovea
The anchor guide was placed through this hole on the femoral neck; a hole was drilled on the cotyloid fossa for insertion of a 2.9 mm anchor loaded with a #2 suture.
This #2 suture was retrieved arthroscopically through the anterolateral portal. One of the suture limbs was passed through a tibialis anterior allograft using a free needle. Then an arthroscopic knot was used to push the graft into the joint through a cannula, until it was compressed against the fossa. A sequence of knots secured this end of the graft at this position (Fig. 30.12a, b).
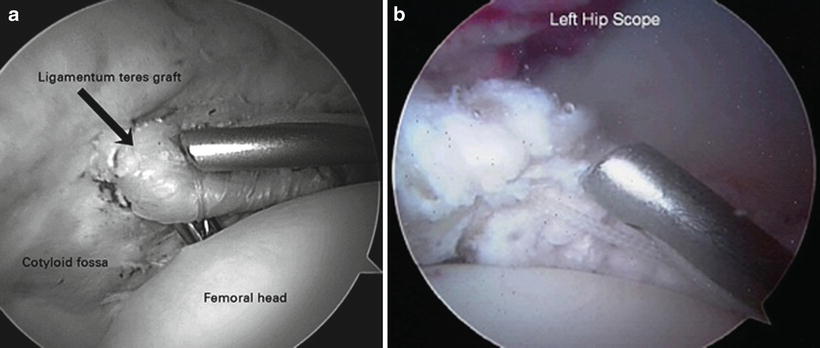
Fig. 30.12
(a, b) Graft is pushed into position with a knot pusher
Then an arthroscopic grasper was inserted through the femoral neck hole to pull the allograft into the femoral neck tunnel. About 2.5 cm of the graft remained between the fovea and the fossa, with the leg in extension and external rotation (Fig. 30.13a, b). This is critical to avoid loss of movement.
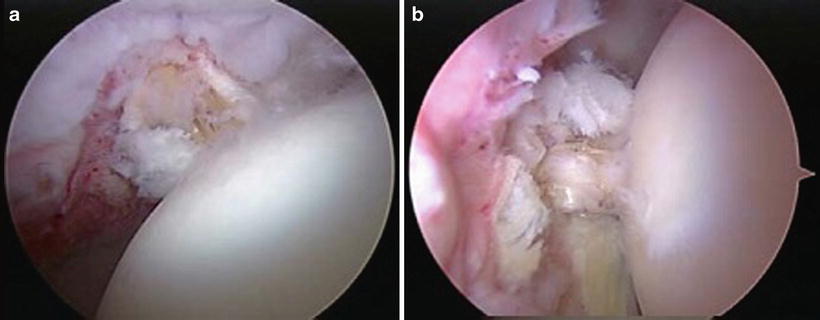
Fig. 30.13
(a, b) Status post fixation of the allograft in position
Tension level was verified by checking the hip’s range of motion and graft excursion. After reaching the desired tension, an 8 × 35 mm interference screw was placed to assure fixation of the graft inside the tunnel. After fixation, the hip range of motion was again verified to be satisfactory.
To end the case, we performed a capsular plication to make sure that the capsule would heal with an appropriate amount of tension, restoring its function as a secondary stabilizer.
Discussion
There are conceptual and technical points to consider upon review of this case. Conceptually, we believe that hip microinstability is multifactorial. The ligamentum teres is a secondary stabilizer of the hip joint. LT insufficiency may become symptomatic in patients with dysplasia and/or following surgical LT debridement. Technically, the LT reconstruction with an allograft needs to be associated with other procedures to address microinstability, such as capsular plication. Meticulous attention should be given to correct allograft length and tension. Reduced length may impair full range of motion. This procedure requires mastery of all advanced hip arthroscopy techniques prior to performance and is presented here as an example of the frontier of treatment in the salvage setting.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


