Chapter 33 Cervical Zygapophysial Joint Nerve (Medial Branch) Injection, Lateral Approach
Note: Please see page ii for a list of anatomical terms/abbreviations used in this book.
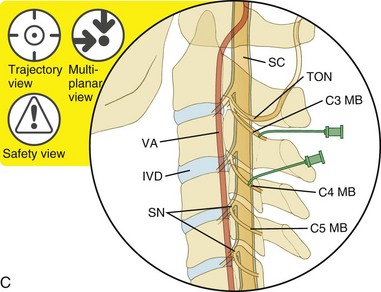
The cervical Z-joints are a well-documented source of acute and chronic neck pain. Symptomatic cervical Z-joints typically produce axial pain. In addition, the upper Z-joints may demonstrate sclerotomal referral patterns that radiate superiorly and anteriorly to involve the head, whereas the lower joints demonstrate patterns that radiate inferiorly and laterally to involve the shoulder and the upper thoracic region.1 The patient’s history, physical examination, and imaging studies will be suggestive of but not specific for Z-joint pain. The standard for the diagnosis of Z-joint pain is either possibly intraarticular Z-joint injection or medial branch blockade.2 Cervical medial branch blocks may have a therapeutic benefit.3 Each Z-joint is innervated by two medial branch nerves. Typically, a lateral projection is best suited for cervical medial branch blockade, especially for the upper segments. The foraminal oblique view (Chapter 3) will assist in visualizing the lower segments, particularly at C7, which may be obscured on a lateral view.
Special attention should be made to Figure 33–10, which illustrates the variability of the cervical medial branch nerves’ anatomical courses.
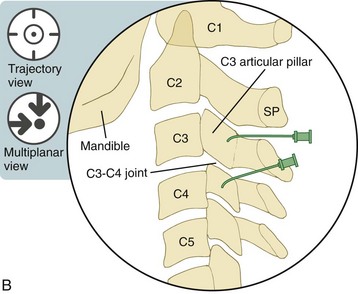
 Trajectory View (Figure 33–1)
Trajectory View (Figure 33–1)
Tilt the fluoroscope cephalad or caudad.


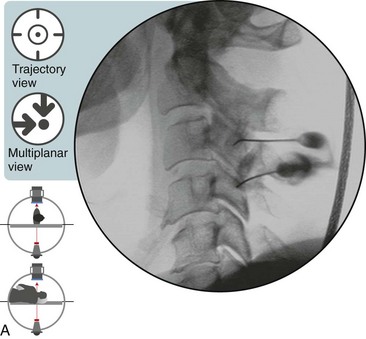
Oblique the fluoroscope minimally (i.e., keep it near neutral).
 Note that a slight degree of obliquity may be required to superimpose the articular pillars to obtain a trapezoid view.
Note that a slight degree of obliquity may be required to superimpose the articular pillars to obtain a trapezoid view.
Confirm the level by counting inferiorly from C2.



 The Trajectory View (Lateral) Is Also a Multiplanar View
The Trajectory View (Lateral) Is Also a Multiplanar View Trajectory View Safety Considerations
Trajectory View Safety Considerations

 Notes on Positioning in the Trajectory View
Notes on Positioning in the Trajectory View

 Optimal Needle Position in Multiplanar Imaging
Optimal Needle Position in Multiplanar Imaging
The multiplanar images include lateral, anteroposterior, and foraminal oblique.
Optimal Needle Positioning in the Lateral View
 For cervical medial branch blocks from the lateral approach, the lateral view is the same as the trajectory view.
For cervical medial branch blocks from the lateral approach, the lateral view is the same as the trajectory view.
Related posts:
 Atlantoaxial Joint Intraarticular Injection
Atlantoaxial Joint Intraarticular Injection
 Lumbar Zygapophysial Joint Nerve (Medial Branch) Radiofrequency Neurotomy, Posterior Approach
Lumbar Zygapophysial Joint Nerve (Medial Branch) Radiofrequency Neurotomy, Posterior Approach
 Cervical Interlaminar Epidural Steroid Injection, Paramedian Approach
Cervical Interlaminar Epidural Steroid Injection, Paramedian Approach
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


