Chapter 23 Thoracic Zygapophysial Joint Intraarticular Injection, Posterior Approach
The needle entry site into the skin is confirmed with anteroposterior visualization at the pedicle one vertebral segment below the designated zygapophysial joint. For example, the entry site in most individuals for a left T8-T9 zygapophysial joint injection is the 6 o’clock position of the left T10 pedicle and the target site for entry into the Z-joint is the 12 o’clock position of the T9 pedicle (Figure 23–1, B). The rationale for the skin entry site and the Z-joint target site is to approximate the “trajectory angle” of the needle tip into the posterior inferior aspect of the joint space due to its near coronal orientation and inability to obtain a trajectory view with fluoroscopy. The needle tip is advanced with fluoroscopy and makes contact with the lamina at the base of the superior articular process of the target Z-joint. The needle tip trajectory is then adjusted and advanced into the Z-joint in the contralateral oblique view.
Note: Please see page ii for a list of anatomical terms/abbreviations used in this book.

 Optimal Needle Position in Multiplanar Imaging
Optimal Needle Position in Multiplanar Imaging
Optimal Needle Positioning in the Anteroposterior View
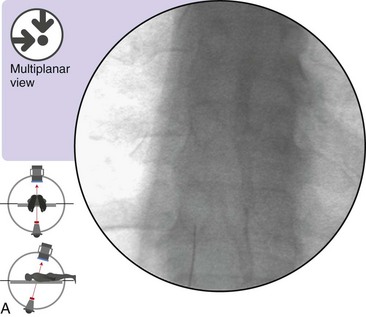
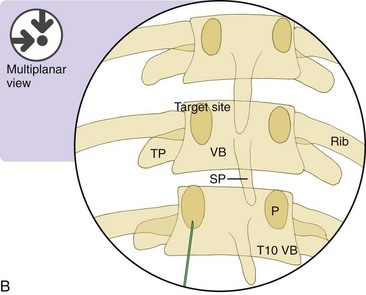
Figure 23–1 A,
Related posts:
 Atlantoaxial Joint Intraarticular Injection
Atlantoaxial Joint Intraarticular Injection
 Lumbar Zygapophysial Joint Nerve (Medial Branch) Radiofrequency Neurotomy, Posterior Approach
Lumbar Zygapophysial Joint Nerve (Medial Branch) Radiofrequency Neurotomy, Posterior Approach
 Cervical Zygapophysial Joint Nerve (Medial Branch) Radiofrequency Neurotomy and Nerve Injection, Posterior Approach
Cervical Zygapophysial Joint Nerve (Medial Branch) Radiofrequency Neurotomy and Nerve Injection, Posterior Approach
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


