Chapter 15 Lumbar Zygapophysial Joint Nerve (Medial Branch) Radiofrequency Neurotomy, Posterior Approach
Note: Please see page ii for a list of anatomical terms/abbreviations used in this book.
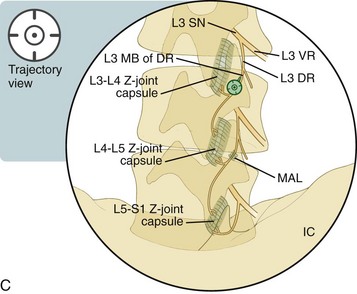
The zygapophysial joints (Z-joints) in the spine are diarthrodial joints with synovial linings that are covered with hyaline cartilage. All Z-joints are innervated by two medial nerve branches: one from the posterior ramus above and one at the same segmental level (e.g., the L3 and L4 medial branches innervate the L4-L5 Z-joint). The only caveat is that the L5-S1 Z-joint is innervated by the L4 medial branch and the L5 dorsal ramus. Please see Figure 14–7 for more details regarding the anatomy of these joints.
Lumbar radiofrequency neurotomy is typically performed after significant pain relief is documented with either an intraarticular Z-joint joint injection and/or a medial branch block injection. However, the approach to lumbar radiofrequency neurotomy is different from the approach used in those injections. In addition, no contrast dye is necessary. The probe is positioned to lay parallel and over the medial branch nerve. Because there is anatomic variation of the course of the medial branch nerve, many practitioners perform, at a mininum, two lesions at each site.1
With the approach described here, the needle is placed with the use of a trajectory view and advanced with the use of multiplanar imaging, with an emphasis on safely using the lateral and ipsilateral oblique views to confirm depth. Before neurotomy, sensory and motor stimulation confirms non-radicular stimulation and 0.5 to 1 cc of anesthetic is typically placed. The time and duration of the denervation varies with different practitioners (e.g., up to three 90-second cycles at 80–85° C).1
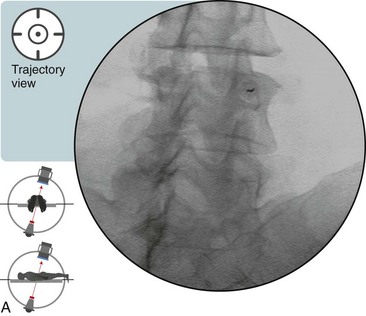
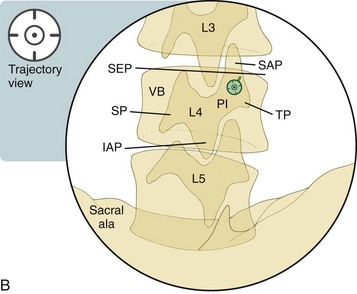
 Trajectory View
Trajectory View








 Optimal Needle Position in Multiplanar Imaging
Optimal Needle Position in Multiplanar Imaging
Related posts:
 Atlantoaxial Joint Intraarticular Injection
Atlantoaxial Joint Intraarticular Injection
 Cervical Zygapophysial Joint Nerve (Medial Branch) Radiofrequency Neurotomy and Nerve Injection, Posterior Approach
Cervical Zygapophysial Joint Nerve (Medial Branch) Radiofrequency Neurotomy and Nerve Injection, Posterior Approach
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


