, Joon Woo Lee1 and Jong Won Kwon2
(1)
Department of Radiology, Seoul National University Bundang Hospital, Seongnam, Kyonggi-do, Republic of Korea
(2)
Department of Radiology, Samsung Medical Center, Seoul, Republic of Korea
12.1 Embryology
12.4 Meningocele
12.5 Myelocystocele
12.7 Dorsal Dermal Sinus
12.8 Diastematomyelia
12.9 Neurenteric Cyst
12.11 Tethered Cord Syndrome
12.13.1 Myelocele/Myelomeningocele
12.13.4 Dorsal Dermal Sinus
12.13.5 Diastematomyelia
12.13.6 Neurenteric Cyst
12.13.7 Caudal Regression Syndrome
12.13.8 Congenital Vertebral Anomalies
Abstract
MR imaging has made the diagnosis of congenital spinal disorders easier, faster, and more accurate. In this chapter, the basic concepts about normal spinal cord embryogenesis are summarized, and the principal congenital malformations (myelomeningocele, lipomyelomeningocele, meningocele, myelocystocele, intradural lipoma, dorsal dermal sinus, and so on) are described. Additionally, several congenital vertebral anomalies are also discussed in this chapter.
MR imaging has made the diagnosis of congenital spinal disorders easier, faster, and more accurate. In this chapter, the basic concepts about normal spinal cord embryogenesis are summarized, and the principal congenital malformations (myelomeningocele, lipomyelomeningocele, meningocele, myelocystocele, intradural lipoma, dorsal dermal sinus, and so on) are described. Additionally, several congenital vertebral anomalies are also discussed in this chapter.
12.1 Embryology
Spinal cord develops through neurulation, canalization, and caudal regression. Neurulation is folding, grooving, and midline fusion of the neural plate to form a neural tube. The brain and the spinal cord are derived from the neural tube. The closure of the neural tube begins in the region of the lower medulla and then proceeds both cephalad and caudad. The neural tube is separated from the overlying ectoderm after the neural tube closure, which is called disjunction. The caudal cell mass, a group of undifferentiated cells at the caudal end of the neural tube, develops microcysts. These microcysts merge together and fuse with the more cephalad portion of the neural tube in a process called canalization. Canalization and retrogressive differentiation of the caudal cell mass result in the formation of conus medullaris, ventriculus terminalis, and filum terminale.
Congenital spinal and spinal cord malformation is referred to as spinal dysraphism (Table 12.1). Myelomeningocele is due to nondisjunction of cutaneous ectoderm from neuroectoderm (open spinal dysraphism) (Table 12.2). Open spinal dysraphism is characterized by exposure of nervous tissue through a congenital defect. Intradural spinal lipoma and lipomyelomeningocele originate from premature disjunction of the cutaneous ectoderm from the neural tube (closed spinal dysraphism). The premature disjunction allows the mesenchyme to penetrate in the neural tube and to contact the primitive ependyma. The penetrating mesenchyme is differentiated into fatty mass. Closed spinal dysraphism is covered by skin. Dorsal dermal sinus is due to defective disjunction.
Caudal regression syndrome, tethered spinal cord, and anterior sacral meningocele belong to anomalies of the caudal cell mass, and diastematomyelia and neurenteric cyst are anomalies of notochord development. Anomalies of vertebral formation and segmentation include hemivertebra, butterfly vertebra, and block vertebra. Atlanto-occipital assimilation is partial or total fusion of the atlas to the occiput.
Table 12.1
Categorization of spinal dysraphisms
1. Open spinal dysraphisms | Myelocele/myelomeningocele |
2. Closed spinal dysraphisms with subcutaneous mass | Lipomyelocele/lipomyelomeningocele |
Meningocele | |
Terminal myelocystocele/myelocytocele | |
3. Closed spinal dysraphisms without subcutaneous mass | Intradural lipoma, fibrolipoma of the filum terminale |
Dorsal dermal sinus | |
Diastematomyelia | |
Neurenteric cyst | |
Caudal regression syndrome |
Table 12.2
Spine congenital anomalies
Causes | Anomalies |
|---|---|
Anomalies of notochord formation | Diastematomyelia, Neurenteric cyst |
Premature disjunction | Intradural lipoma, lipomyelocele, lipomyelomeningocele |
Nondisjunction | Myelocele, myelomeningocele |
Defective disjunction | Dorsal dermal sinus |
Abnormal caudal cell mass | Tight filum terminale syndrome |
Fibrolipoma of the filum terminale | |
Caudal regression syndrome | |
Anterior sacral meningocele | |
Sacrococcygeal teratoma | |
Unknown origin | Myelocystocele, meningocele |
12.2 Myelocele/Myelomeningocele
Myelocele and myelomeningocele result from a failure of neurulation and are characterized by exposure of the neural placode through a large defect in the midline of the low back to the environment. In the myelomeningocele, herniation of the sac of the exposed placode occurs due to expansion of the underlying subarachnoid space. The spinal cord is tethered posteriorly at this level. In myelocele or myeloschisis, however, the placode is flush with the plane of the back and identifiable on the cutaneous surface. Because the exposed placode is ulcerated and infected, the mortality is very high in the untreated newborn. Because these newborns are usually operated on soon after birth, MRI is rarely performed prior to surgery. Associated anomalies are Chiari II malformation, hydrocephalus, syringomyelia, and inclusion dermoid or epidermoid cyst.
12.3 Lipomyelocele/Lipomyelomeningocele
Lipomyeloceles and lipomyelomeningoceles are caused by premature disjunction of the neural tube and the cutaneous ectoderm and manifest as a subcutaneous fatty mass in the paramedian of the lower back.
MR imaging will show an intraspinal lipomatous mass that extends to the subcutaneous fat through a posterior bony defect of the lumbosacral spine. The mass is connected to the spinal cord, which may be low lying or tethered. The spinal canal is widening depending on the size of the lipomatous mass, and there may be other anomalies such as sacral agenesis. Expansion of the intradural space may result in prolapse of meninges through the large posterior bony defect (posterior meningocele). Lipomyelocele combined with posterior meningocele is referred to as lipomyelomeningocele. Lipomyelomeningocele is usually present at birth and is diagnosed before neurologic signs develop. After lipomyelomeningocele repair, however, recurrent tethering of the spinal cord requiring further operative intervention may develop. If the patients with lipomyelomeningocele present new symptoms after operation, repeated MR imaging should be performed to rule out retethering.
12.4 Meningocele
Meningocele is protrusion of the meninges through a bony defect forming a cyst filled with cerebrospinal fluid. It is covered with skin and does not contain neural tissue. The most common sites are lumbar and sacral locations, and occipital or cervical location can be possible.
12.5 Myelocystocele
Myelocystocele is herniation of large terminal syrinx into the posterior meningocele, forming a skin-covered cystic mass. The spinal cord is low lying and tethered. The cyst has ependymal lining. The inner terminal cyst (myelocystocele) communicates with the central canal of the spinal cord, and the outer dural sac (meningocele) communicates with the subarachnoid space. The outer and inner fluid spaces usually do not communicate. Myelocystocele can be associated with cloacal anomaly or partial sacral agenesis.
12.6 Intradural Lipoma/Fibrolipoma of the Filum Terminale
Intradural lipomas are associated with spinal dysraphism and comprise less than 1 % of primary spinal tumors. Intradural lipomas consist of mature fat cells separated by connective tissue strands and are histologically identical to normal body fat. The size of the lipomas may increase while the patients are growing up or in particular conditions such as obesity or pregnancy. Intradural lipomas are commonly located in the cervicothoracic spine and can cause slow progression of spinal cord compression. Lumbosacral lipomas and usually present with the tethered cord syndrome. Intradural lipomas appear as round or lobulated masses that demonstrate isointense to subcutaneous fat on all MR sequences including fat-saturated or short tau inversion recovery (STIR) images (Tortori-Donati et al. 2000, 2001). The adjacent spinal cord is compressed and may show compressive myelopathy, hyperintense on T2-weighted image.
Fibrolipoma of the filum terminale is caused by incomplete retrogressive differentiation of the caudal cell mass. Neurologic and orthopedic deformities can be associated with fibrolipoma of the filum terminale, and the spinal cord is usually low lying.
12.7 Dorsal Dermal Sinus
Dorsal dermal sinus is an epithelium-lined tract that extends from the skin surface to the spinal cord and the meninx. It is found more frequently in the lumbosacral region. The cutaneous abnormality is usually detected at birth. Unrecognized patients, however, can develop complications such as meningitis or cord abscesses. Dorsal dermal sinuses can be associated with dermoid, epidermoid, and lipoma.
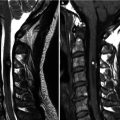
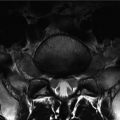
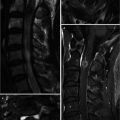
12.8 Diastematomyelia
Diastematomyelia is caused by failure of midline integration of the notochord and results in elongated separation of the spinal cord and/or cauda equina along a midsagittal plane (i.e., split cord malformation). Each hemicord has one central canal, one dorsal horn, and one ventral horn and originates the ipsilateral dorsal and ventral nerve roots. The two hemicords usually rejoin into a single cord below the level of the separation. Most of the cleft occurs between T9 and S1.
Diastematomyelia type I consists of two hemicords, separated by a fibrous or osteocartilaginous septum that extends from the vertebral body posteriorly to the neural arches (Pang et al. 1992). Each hemicord has dural sac and subarachnoid space. Diastematomyelia type II is characterized by two hemicords in single dural sac and arachnoid space. Type II doesn’t have an osteocartilaginous spur to divide the spinal canal. Patients with type II may have a less severe neurologic impairment than those with type I.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


