Disorders of the Wrist
Ulnar Side
Tendon Disease
Extensor Carpi Ulnaris Instability
The subsheath may be normally visualized at ultrasound as a thin curvilinear hypoechoic structure overlying the tendon.
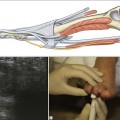
Dynamic scanning of ECU in short axis is used to demonstrate volar subluxation of the tendon with forearm supination and wrist flexion (Fig. 12.1).

Figure 12.1 ECU instability. Transverse images show (A, B) the ECU normally situated in the ulnar groove (arrowheads) with the wrist in the neutral position and (C, D) progressive flattening and volar dislocation of the ECU tendon out of the ulnar groove (arrowheads) with forearm supination and wrist flexion.
Permanent dislocation of the tendon is uncommon and is best seen in the transverse plane over the posteromedial ulna. The ulnar groove is empty and the retinaculum is usually attenuated and irregular.
ECU Tenosynovitis
ECU tenosynovitis is mostly due to mechanical friction of the tendon against the ulna, secondary to instability. Patients present with localized pain over the dorsal medial aspect of the distal ulna and occasionally a snapping sensation if tendon subluxation is present. Ultrasound is valuable to identify a tendon sheath effusion and synovial hypertrophy, associated tendinosis and intratendinous splits (Fig. 12.2), as well as tendon subluxation (Figs 12.3 and 12.4).

Figure 12.2 There is a longitudinal split in the ECU tendon. A little fluid is present in the tendon sheath.

Figure 12.3 ECU tenosynovitis and instability. Transverse image demonstrates volar subluxation of the ECU tendon over the ulnar border (arrow) of the ulnar groove. Mechanical friction of the tendon against the ulna results in ECU tenosynovitis with a tendon sheath effusion and synovial hypertrophy (arrowheads).

Tenosynovitis of Other Extensor Tendon Compartments
All of the extensor compartments (ECs) may be affected by tenosynovitis and tendinopathy, although EC4 and EC5 are least common. EC4 is normally surrounded by a thick retinaculum, much thicker than the other compartments. This should not be misinterpreted as tenosynovitis. True tenosynovitis will fill the compartment unevenly (Fig. 12.5) and may be accompanied by increased Doppler activity in many cases (Fig. 12.6). Furthermore, intrasheath synovitis will result in some separation of the tendons.

Figure 12.5 Sagittal image of dorsal aspect of wrist. Thickened synovium and synovial exudate distend the common extensor sheath. The extensor tendon visualized appears normal.