Chapter 15 Thoracic skeleton
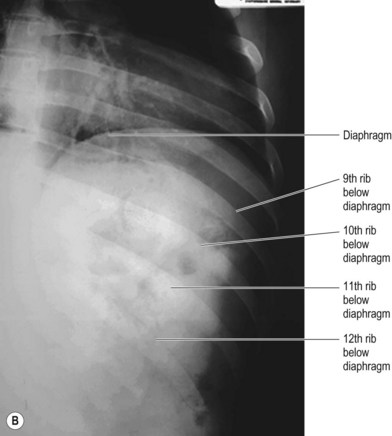
The bones of the thorax consist of the ribs and sternum, but radiographic examination of the area also involves demonstration of the sternoclavicular (SC) joints. Referrals for radiography of the ribs have declined, especially in cases of trauma. Although painful, rib fractures are treated conservatively unless displacement causes fracture fragments to penetrate the soft issue of the thorax and induce pneumothorax or haemothorax. Evidence of these conditions is definitely required via radiographic examination, but the posteroanterior (PA) chest projection is considered to be the most appropriate means for demonstration of these appearances,1 as the most important aspect of diagnosis is that of assessing the effect injury may have had on thoracic contents. The PA chest film is also very likely to demonstrate the fractured rib and fragments causing a pneumothorax, haemothorax or evidence of visceral damage.2,3 Ribs positioned below the diaphragm on the PA image are those that are less likely to penetrate the pleura, thus reducing or eradicating the need for separate X-ray examination of these. The PA chest image also shows ribs 1–6 reasonably well in their entirety, but not ribs 7–12.
Metastatic deposits may be demonstrated by X-ray but are better located via scintigraphy; however, as metastases in the rib may lead to pathological fracture it may be necessary to undertake plain radiography. In addition to fractures and metastasis, other rib lesions seen on plain radiography include fibrous dysplasia, aneurysmal bone cysts, myeloma and granuloma,4 but it is questionable whether X-ray would be the method of choice to demonstrate them.
Oblique ribs
Posterior oblique for upper ribs (Fig. 15.1A,B)

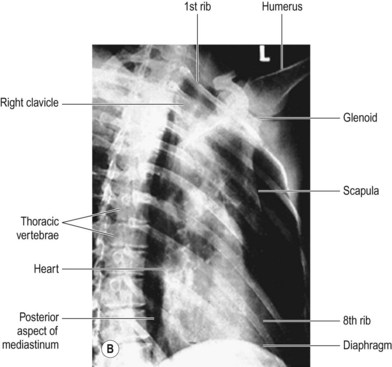
Figure 15.1 Posterior oblique – upper ribs.
(B) Reproduced with permission from Bryan GJ. Skeletal anatomy. 3rd ed. Edinburgh: Churchill Livingstone; 1996 and Gunn C. Bones and joints. 4th ed. Edinburgh: Churchill Livingstone, 2002.
Positioning
• A lead rubber apron is applied to the patient’s waist
• The patient stands with their back to the IR and faces the X-ray tube; the side under examination is positioned with the lateral borders of ribs 1–6 well within the IR border
• The arm on the side under investigation is raised and the forearm rested on the head; this will clear the arm from the area of interest
• The patient is rotated 30–45° towards the side under examination; the thorax on the side of interest rests against the IR
Beam direction and focus receptor distance (FRD)
Beam is initially horizontal, with 12° caudal angulation
Centring
Two-thirds of the way down the line adjoining sternal notch and xiphisternum
IR displacement may be required to ensure that the area of interest lies within its boundaries
Collimation
C7 to T12, lateral margins of ribs on affected side, midclavicular line on the opposite side
Traditionally the upper rib oblique projection has been described using antiscatter grid,5,6 but as ribs 1–6 lie superior to the diaphragm in a low-density area, direct exposure is possible without an antiscatter device. This allows reduction in exposure factors and therefore affords less radiation dose to the patient. In the case of larger patients it is possible that provision of adequate contrast may be compromised by an increase in tissue density. This, coupled with the higher density over the mediastinum, may require the use of a grid.
Criteria for assessing image quality
• The entire length of ribs 1–6 are demonstrated above diaphragm
• Heart shadow may overlie medial aspect of sixth rib in the case of right-sided ribs, or most of the sixth rib in the case of left-sided ribs
• Oblique appearance of thoracic vertebrae
• Image of anterior ribs moved laterally in comparison to their position as seen on the PA chest image
• Sharp image demonstrating ribs in contrast to air-filled lung tissue and viscera of the mediastinum and heart
| Common errors | Possible reasons |
|---|---|
| High-contrast image which does not demonstrate ribs in contrast to viscera and heart | kVp selected is too low. It will be necessary to compensate for kVp increase by reducing mAs proportionally to avoid over-blackening over the lung area |
| Over-blackened image generally | If automatic exposure chamber used, the central ray and chamber selected may be lying over the dense mediastinum |
| Pale shadow overlying lateral ribs | Arm not cleared from area |
| Lower ribs (4–6) pale and shown below diaphragm | Exposed on expiration |
Posterior oblique for lower ribs (Fig. 15.2A,B)
Positioning
• A lead rubber apron is applied to the patient’s waist
• The patient stands with their back to the IR and faces the X-ray tube; the side under examination is positioned with the lateral borders of ribs 7–12 well within the IR boundaries
• The arm on the side under investigation is raised and the forearm rested on the head; this will clear the arm from the area of interest
• The patient is rotated 30–45° towards the side under examination; the thorax on the side of interest rests against the IR