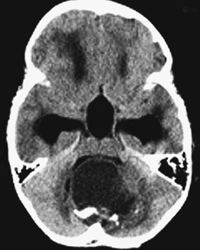
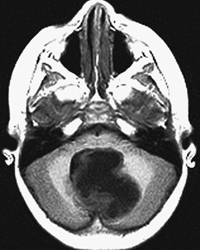
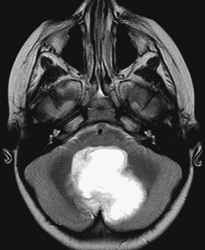
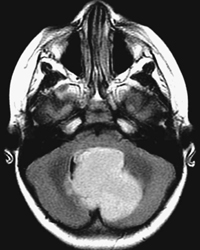
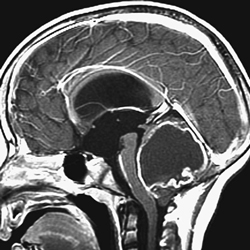
CASE 1 A child presents with vomiting, headaches, and, later, personality changes. Figure 1A Figure 1B Figure 1C Figure 1D Figure 1E Figure 1F Initial CT without contrast demonstrated dilated third ventricle and temporal horns (with compressed hippocampi) (Fig. 1A). A large, rounded hypodense mass is noted behind the fourth ventricle, in the vermis and adjacent portions of the cerebellar hemispheres. This mass appears cystic with two solid mural nodules, one anterior on the left and the other posterior on the right with calcification. Nonenhanced MR images show similar findings with low T1 (Fig. 1B) and high T2/FLAIR (Figs. 1C and 1D). The cyst content presents attenuation and signals different from the adjacent CSF. Following contrast, MRI (Figs. 1E and 1F) demonstrates enhancement of the cyst wall and of the solid mural nodules. Note the anterior third ventricle bulging into a large cisternal space (presurgical ventriculocisternotomy possible to alleviate hydrocephalus) and the tonsillar herniation through the foramen magnum (risk of acute compression of the medulla). Cerebellar juvenile pilocytic astrocytoma (JPA)
Clinical Presentation

Radiologic Findings
Diagnosis
Differential Diagnosis
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


