10 Spleen
The spleen is a pyramid-shaped organ normally located in the left upper quadrant. It forms part of and is the largest organ within the lymphoproliferative system. It plays a major role in the immune system and also functions as a filter of damaged and abnormal red blood cells.
Imaging of the spleen starts and often rests very much with ultrasound. Depending on a child’s age, this organ can be imaged with transducers of different frequencies. Exquisite images can be obtained with higher frequency, particularly in the younger child.
Requests for examining this organ are often related to a clinically palpable increase in its size. Other frequent indications are for the assessment of hematologic conditions and in the setting of trauma. The assessment and measurement of the spleen are part of the normal ultrasound examination of the pediatric abdomen.
This chapter describes the normal appearances, variants, and most common pathologies of the spleen as seen with ultrasound.
10.1 Normal Anatomy and Variants
10.1.1 Embryology
The spleen begins to develop at the fifth week of fetal life. It develops from multiple cellular nests located within the dorsal mesogastrium ( Fig. 10.1 ). Symmetrical splenic precursors are thought to exist with preferential development of the left sided splenic tissue. These cellular nests eventually fuse to form a single organ. The small anterior notch often seen in the anterior aspect of the spleen is thought to result from this fusion process. The presence of accessory small spleens (splenunculi), seen in about 10% of normal individuals, results from incomplete fusion of all the splenic tissue into one organ.
Given its embryonal development in the dorsal mesogastrium, the final location of splenic tissue is very much dependent on normal situs and normal bowel rotation. At 8 weeks’ gestation, the liver rotates to the right, and the stomach and spleen rotate to the left. The peritoneal reflections between these organs follow their rotational movement.

10.1.2 Anatomical Considerations
The final anatomical splenic position and the layout of its associated peritoneal reflections are demonstrated in Fig. 10.2 . The spleen is surrounded by peritoneum, with folds that meet in positions anterior and posterior to the organ. The gastrosplenic ligament connects the spleen with the greater curvature of the stomach anteriorly. The lienorenal ligament in turn connects the spleen to the retroperitoneum posteriorly. The tail of the pancreas is partly located within this latter peritoneal reflection and can be easily seen in close relation to the splenic hilum on ultrasound. The splenic hilum effectively points medially between the stomach and the left kidney, both of which leave an indentation. Medial to the gastrosplenic and lienorenal ligaments is the lateral aspect of the lesser sac of the peritoneal cavity. Further peritoneal reflections run from the spleen superiorly to the diaphragm (phrenicosplenic ligament) and inferiorly to the colon (splenocolic ligament).

Superiorly, the spleen is related to the diaphragm, lying in a concavity within the left hemidiaphragm. Anteriorly, the organ is related to the stomach and left colon. Posteriorly lie the diaphragm, left pleura, lung base, and chest wall.
Arterial blood supply comes through the splenic artery, which is a branch of the celiac trunk of the aorta. This courses behind the pancreas and reaches the spleen through the lienorenal ligament. The splenic artery divides into a number of branches before entering the spleen. This is described to follow two main patterns. In the distributed type (70%), the primary trunk is short and many long branches reach the splenic hilum. Alternatively, in the magistral type (30%), the main trunk is long with short arterial branches at the hilum. The splenic vein forms in the lienorenal ligament from venous tributaries, which leave the spleen at the hilum. The unified vein travels with the artery behind the pancreas to join with the superior mesenteric vein and form the portal vein.
Histologically, the spleen is formed by a fibrous capsule that supplies a network of trabeculations serving as a supportive framework for the functional tissue. The functional tissue consists of two types. The white pulp (which derives its name from its appearance on gross pathology specimens) consists of groups of lymphocytes and lymphoid follicles. The red pulp comprises the remainder of the spleen (approximately 75% of the volume) and is composed of venous sinusoids through which the blood slowly filters.
10.1.3 Technique and Normal Ultrasound Appearances
On interrogation with ultrasound, the normally located spleen is identified in the left upper quadrant, above the left kidney and under the left hemidiaphragm, either through a window under the left lower rib margin or through the lower intercostal spaces. Images should be obtained in the transverse and coronal oblique planes along the length of the organ ( Fig. 10.3 and Fig. 10.4 ). These images can generally be obtained in the supine position, although rotating the child into the lateral decubitus position ( Fig. 10.5 ) can assist in obtaining a suitable window when imaging in the supine position is proving difficult. Occasionally, the lung and pleura can partially obscure the superior aspect of the spleen. The examiner can ask compliant children, particularly older children, to hold their breath briefly in expiration while he or she gently slides the probe up and down the lower left intercostal spaces until the organ comes into view ( Fig. 10.6 ; Video 10.6).




10.1.4 Echogenicity and Changes in Echogenicity with Age
As a rule of thumb, the spleen is expected to have echogenicity similar to that of the liver and appear more echogenic than the adjacent kidney. This is assuming that the hepatic and renal echogenicity is normal when these organs are used as a comparison for assessing the echogenic appearance of the spleen.
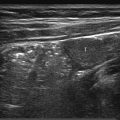
The spleen appears diffusely homogeneous. When it is evaluated with higher-frequency probes, the echotexture can appear rather heterogeneous, and this finding should not be misinterpreted as pathology ( Fig. 10.7 ). The degree of heterogeneity ranges from mild granularity to better-defined tiny areas of hypoechogenicity throughout the organ. Some authors have clearly demonstrated that these heterogeneous appearances change with age and are best identified in children between the ages of 1 and 5 years. Such appearances are attributed to the presence of white pulp/lymphoid follicles in the spleen, which are thought to account for the tiny focal areas of low echogenicity described.

The inability to demonstrate such heterogeneity in infants is thought to result from the immaturity of the organ at this tender age. Difficulty in seeing such detail in older children may result from their increased size, reducing the resolution obtained, although the literature indicates that the chances of demonstrating such heterogeneity increases both with age and with organ size.
It is very important to become comfortable with normal splenic appearances at different frequencies and with the various probes that are part of one’s regular equipment.
10.1.5 Vascularity
When interrogated with color Doppler ultrasound, the spleen appears hyperemic. The splenic artery is seen to arise from the celiac trunk and can be followed along its course behind the pancreas into the lienorenal ligament and splenic hilum, where its branches can be identified ( Fig. 10.8 ). Similarly, the draining venous tributaries are seen in the splenic hilum forming the splenic vein. This can be followed behind the pancreas close to the artery to its junction with the superior mesenteric vein ( Fig. 10.9 ).


10.1.6 Normal Variants
Splenunculi
In around 10% of healthy individuals, failure of all the embryonic splenic tissue to join and form a single spleen may result in the presence of a small round or oval area of normal splenic tissue adjacent to the main splenic organ, known as an accessory spleen or splenunculus. If multiple areas are present, these are referred to as splenunculi ( Fig. 10.10 ). These are often identified incidentally on scanning. Their echogenicity is similar to that of the main spleen. Splenunculi derive their blood supply from branches of the splenic artery.

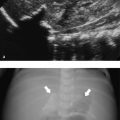
Splenunculi are common and often of no clinical significance. They rarely can present with torsion and infarction ( Fig. 10.11 ). They can also significantly enlarge and become hypertrophic, assuming the function of the larger spleen, in hematopoietic conditions after a splenectomy, resulting in recurrent hypersplenism.

Splenic Notch
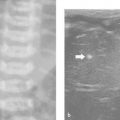
A small notch/cleft can occasionally be identified on the medial aspect of the undersurface of the spleen ( Fig. 10.12 ). This is thought to be a remnant from the fusion of the splenic nests of tissue during embryonal development. This is easier to appreciate in cross-sectional imaging than with ultrasound. In the context of trauma, the notch can be mistaken for a peripheral laceration. However, one would expect some free fluid/hemoperitoneum adjacent to such a finding in the case of an acute traumatic laceration.

10.1.7 Normal Splenic Size
The spleen grows with the growing child. Normal data are available for splenic length in premature infants, neonates, and older children ( Table 10.1 and Table 10.2 ). Fig. 10.13 demonstrates the appropriate method of measuring the spleen in the coronal plane. At birth, the spleen measures between 2.5 and 4.9 cm in length. At full growth, the spleen is expected to measure between 8.7 and 11.0 cm in a girl and 9.5 and 12.5 cm in a boy.

Splenic length (cm) | |||
Gestational age (weeks) | No. of patients | Mean length (± 1 SD) | Minimum–maximum |
24–31 | 29 | 2.4 (0.4) | 1.6–3.2 |
32–35 | 34 | 2.8 (0.5) | 1.7–4.0 |
36–37 | 35 | 3.3 (0.4) | 2.6–4.2 |
38–41 | 155 | 3.4 (0.5) | 2.4–4.9 |
Abbreviation: SD, standard deviation. Source: Reprinted with permission of Elsevier from Soyupak SK, Narli N, Yapicioglu H, Satar M, Aksungur EH. Sonographic measurements of the liver, spleen and kidney dimensions in the healthy term and preterm newborns. Eur J Radiol 2002;43(1):73–78. Note: This study was performed in 261 healthy newborn infants. Craniocaudal dimensions of the spleen were determined with ultrasonography. | |||
Spleen length (cm) | Spleen length (cm) | ||||||||
Age and sex | Number | Mean | SD | Min-max | Age and sex | Number | Mean | SD | Min-max |
Age and sex | Number | Mean | SD | Min-max | Age and sex | Number | Mean | SD | Min-max |
0–3 mo | 6–8 y | ||||||||
F | 22 | 4.4 | 0.57 | 3.2–5.5 | F | 25 | 8.2 | 0.99 | 6.6–10.0 |
M | 35 | 4.6 | 0.84 | 2.8–6.8 | M | 26 | 8.9 | 0.91 | 7.4–10.5 |
3–6 mo | 8–10 y | ||||||||
F | 6 | 5.2 | 0.47 | 4.5–5.6 | F | 26 | 8.7 | 0.92 | 6.4–10.5 |
M | 10 | 5.8 | 0.65 | 4.9–7.0 | M | 15 | 9.0 | 1.02 | 7.4–11.2 |
6–12 mo | 10–12 y | ||||||||
F | 15 | 6.3 | 0.68 | 5.1–7.5 | F | 34 | 9.1 | 1.09 | 6.8–11.4 |
M | 12 | 6.4 | 0.78 | 5.4–7.4 | M | 19 | 9.8 | 1.05 | 7.3–11.3 |
1–2 y | 12–14 y | ||||||||
F | 18 | 6.3 | 0.69 | 5.1–8.2 | F | 30 | 9.8 | 1.02 | 7.9–11.6 |
M | 17 | 6.8 | 0.72 | 5.6–8.3 | M | 18 | 10.2 | 0.81 | 8.5–11.7 |
2–4 y | 14–17 y | ||||||||
F | 24 | 7.5 | 0.83 | 5.7–8.9 | F | 13 | 10.3 | 0.69 | 8.7–11.0 |
M | 22 | 7.6 | 1.07 | 5.9–9.9 | M | 13 | 10.7 | 0.90 | 9.5–12.5 |
4–6 y | |||||||||
F | 36 | 8.0 | 0.74 | 6.7–9.5 | |||||
M | 18 | 8.1 | 1.01 | 6.4–9.9 | |||||
F, female; M, male; SD, standard deviation. | |||||||||
Permission to reuse from Megremis SD, Vlachonikolis IG, Tsilimigaki AM. Spleen length in childhood with US: normal values based on age, sex, and somatometric parameters. Radiology 2004;231:129–134. © Radiological society of North America. | |||||||||
Tips from the Pro
The spleen should be assessed systematically in two planes. Always measure and document the craniocaudal length of the spleen. Do get into the habit of assessing the splenic echotexture with a higher-frequency probe. Although this may not allow the full depth of the spleen to be assessed, it provides great views of the echotexture and makes it possible to detect subtle lesions that, when small and diffuse, may not be seen with standard probes and settings. Do not mistake the normal heterogeneity seen with higher-frequency probes for pathology.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


