11 Selected Interesting SPECT and SPECT/CT Cases
11.1 Introduction
This chapter provides several illustrative cases in which single-photon emission computed tomography (SPECT) and/or SPECT/computed tomography (SPECT/CT) was helpful in achieving an accurate diagnosis. We have included two types of cases: (1) cases where SPECT and/or SPECT/CT is commonly performed in clinical practice but that illustrate points which have not been discussed elsewhere in this book and (2) cases for which the role of SPECT and/or SPECT/CT is not well established but rather is performed as needed. For example, SPECT and/or SPECT/CT is not commonly done for examinations requiring dynamic imaging (e.g., cholescintigraphy or gastrointestinal bleeding studies) but may be extremely valuable in certain cases.
11.2 Case 1: Incidental Retrosternal Goiter Found on Myocardial Perfusion SPECT
11.2.1 Clinical History and imaging Findings
An 80-year-old woman presented with shortness of breath.
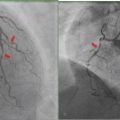
Technetium-99 m (99mTc)-sestamibi myocardial perfusion imaging (MPI) was performed following pharmacological stress to evaluate for cardiac disease.
SPECT images in short axis (SA), vertical long axis (VLA), and horizontal long axis (HLA) demonstrate normal myocardial perfusion (► Fig. 11.1 a).
The raw data reveal a large area of increased radiotracer activity in the anterior mediastinum (arrow) that was confirmed to be a retrosternal goiter on surgery (► Fig. 11.1 b).

11.2.2 Teaching Points
Careful attention should be paid to identify noncardiac as well as cardiac findings on MPI. In some cases, these findings may account for the patient’s symptoms. Systematic review of the raw data is helpful not only to detect quality control issues but also to identify noncardiac incidental findings.
Extracardiac thoracic uptake may be due to benign or malignant disease. For example, lung cancer, breast cancer, lymphoma, sarcoidosis, and vascular abnormalities may be identified, among other things. Thymic uptake, a retrosternal goiter, and skeletal uptake in multiple myeloma are some other conditions that can be seen by reviewing the raw data. 1 , 2
11.3 Case 2: Myocardial Viability Assessment with Thallium
11.3.1 Clinical History and Imaging Findings
A 62-year-old woman presenting with ischemic cardiomyopathy and marked left ventricular contractile dysfunction underwent thallium-201 (201Tl) SPECT for assessment of myocardial viability.
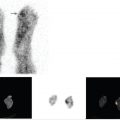
Initial resting SPECT images (top row) on SA, VLA, and HLA demonstrate a large size, moderate to severe intensity perfusion defect in the anterior, apical, and inferolateral walls, corresponding to the vascular territory of the left anterior descending and left circumflex coronary arteries (► Fig. 11.2).
Redistribution images at 4 hours (Fig. 11.2, bottom row) demonstrate significant redistribution of 201Tl activity consistent with hibernating myocardium in both vascular territories. These findings suggest a high likelihood that this patient would benefit from a revascularization procedure.

11.3.2 Teaching Points
“Hibernating” myocardium is viable tissue with contractile dysfunction due to hypoperfusion. Myocardial viability assessment is very important when planning a revascularization procedure in high-risk surgical patients. While fluorine-18 fluorodeoxyglucose (FDG) cardiac positron emission tomography (PET) is considered to be the gold standard test to identify hibernating myocardium, PET may not always be accessible, in which case 201Tl SPECT may be an attractive alternative test.
201Tl is a potassium analogue that is injected as thallous chloride and enters myocytes via active transport involving the Na + /K + adenosine triphosphate transport system. From the intracellular space, 201Tl then washes back out into the systemic circulation. In general, 201Tl clears more slowly from myocardium supplied by stenotic vessels than from myocardium that is normally perfused. Hypoperfused areas may continue to accumulate thallium intracellularly, with resultant redistribution. 3
11.4 Case 3: Hepatic Hemangioma
11.4.1 Clinical History and imaging Findings
A 53-year-old man with left-sided abdominal pain had a diagnostic CT that showed a liver mass with features suggestive of but not definitive for a hepatic hemangioma.
A 99mTc-labeled red blood cell (RBC) SPECT study was performed for further evaluation of the liver mass.
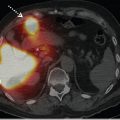
SPECT images show a large area of abnormal radiotracer accumulation in the region of the left hepatic lobe corresponding to the mass on CT (► Fig. 11.3 a). The delayed radiotracer uptake is heterogeneous with relative photopenia centrally and intense radiotracer uptake peripherally.
Fused diagnostic CT and SPECT images show radiotracer uptake predominantly along the periphery of the lesion (► Fig. 11.3 b). The scintigraphic appearance is consistent with a hepatic hemangioma.

11.4.2 Teaching Points
Hemangiomas, focal nodular hyperplasia, and inflammatory pseudotumors of the liver are the common regenerative hepatic lesions. The most common benign hepatic tumor is the hemangioma, which is usually discovered incidentally and has an uncomplicated course. It is important to differentiate hemangiomas from other lesions, such as metastases, in order to avoid unnecessary investigations and/or treatment.
Immediate 99mTc-RBC blood pool images often show decreased activity in a cavernous hemangioma. Heterogeneous activity is seen on imaging obtained 1 to 2 hours after radiotracer administration. Often there is increased activity peripherally and central photopenia related to thrombosis, fibrosis, and/ or necrosis.
The specificity and positive predictive value of both planar and SPECT 99mTc-RBC blood pool imaging is virtually 100% in diagnosing hepatic hemangioma. Planar imaging alone can identify large lesions (e.g., > 3 cm) with a low overall sensitivity of 30 to 53%. The sensitivity of SPECT 99mTc-RBC blood pool imaging is higher but still heavily dependent on lesion size and, to some degree, technique; overall sensitivity is 70 to 80% using single-head SPECT. Using multihead cameras, the sensitivity ranges from 17 to 20% for the detection of lesions < 1 cm, 65 to 80% for lesions 1 to 2 cm, and virtually 100% for lesions ≥ 1.4 cm.
SPECT/CT improves the sensitivity further, especially when lesions are small or located adjacent to vascular structures. 4 , 5 , 6
11.5 Case 4: Peritoneal Scintigraphy
11.5.1 Clinical History and imaging Findings
A 59-year-old man with end-stage renal disease on peritoneal dialysis presented with sudden onset of scrotal swelling and pain.
Peritoneal scintigraphy was performed after injection of 99mTc-labeled sulfur colloid mixed with peritoneal dialysate into the peritoneal cavity.
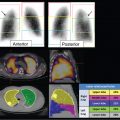
Initial planar images centered over the abdomen (left) and pelvis including the scrotum (right) show diffuse radiotracer activity in the peritoneal cavity and asymmetric radiotracer uptake extending inferiorly in the region of the scrotum (► Fig. 11.4 a).
Coronal SPECT images show the radiotracer extending through the right inguinal canal into the scrotum (► Fig. 11.4 b). Focal photopenia surrounded by tracer within the right scrotum most likely represents the right testicle.
Fused axial, sagittal, and coronal SPECT/CT images confirm radiotracer movement through the right inguinal canal into the scrotum consistent with an abnormal peritoneoscrotal communication and dialysate leak (► Fig. 11.4 c). Peritoneal dialysis was discontinued with initiation of hemodialysis, and the inguinoscrotal communication was surgically repaired.

11.5.2 Teaching Points
A dialysate leak can occur as a result of a peritoneal membrane tear, where loss of peritoneal membrane integrity may be induced by increased intra-abdominal pressure when large volumes of dialysate are infused during peritoneal dialysis.
Dialysate leaks are classified as early and late based on the time of symptom onset following peritoneal catheter insertion.
A dialysate may leak as follows:
Into the abdominal wall through a peritoneal defect, presenting as abdominal wall swelling.
Into the pleura via an abnormal peritoneal–pleural communication, causing a pleural effusion.
Into the scrotum through a patent processus vaginalis, presenting as inguinoscrotal swelling with pain.
At the catheter insertion or exit site, presenting as subfascial or subcutaneous swelling with or without pain. 7 , 8
An advantage of peritoneal scintigraphy is the ability to obtain delayed images, even up to 24 hours, allowing more time for the radiotracer to reach the leak or hernia. The addition of SPECT/ CT can help pinpoint the exact location of the peritoneal leak. SPECT/CT can be useful in establishing an unequivocal diagnosis of peritoneal leak. 8
11.6 Case 5: Pseudoaneurysm
11.6.1 Clinical History and Imaging Findings
A 70-year-old man presented with coronary artery disease, peripheral vascular disease, and multiple prior vascular interventions.
A 99mTc-HMPAO-labeled white blood cell (WBC) scan was performed for evaluation of unexplained fever.
Whole-body planar images show mild asymmetric increased radiotracer activity in the region of the right femoral head and neck, which prompted further evaluation with SPECT/CT (► Fig. 11.5 a).
Axial SPECT at the level of the hips shows focal activity in the right inguinal region (► Fig. 11.5 b).
Fused SPECT/CT confirmed the increased radiotracer accumulation in the right inguinal region was in a pseudoaneurysm, consistent with an infected pseudoaneurysm (► Fig. 11.5 c).

Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


