Magnetic resonance imaging (MRI) is far superior to computed tomography (CT) for the visualization of soft tissue pathology because of greater soft tissue contrast and an overall improved tissue characterization based on signal behavior on different pulse sequences and relaxation parameters. Compared with MRI, CT is more sensitive for the diagnosis of both tiny soft tissue calcifications and air collections and facilitates differentiation between the two.
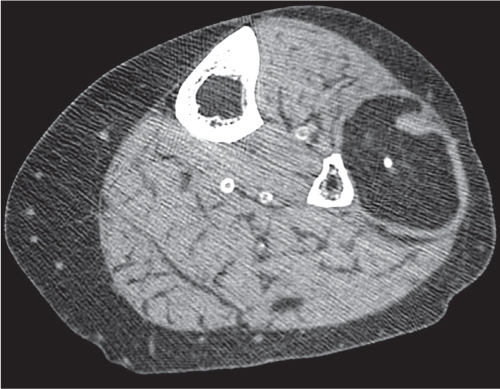
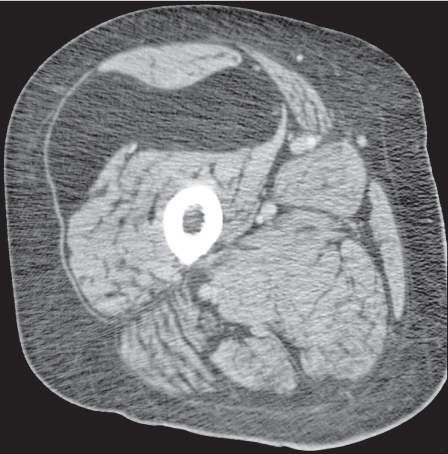
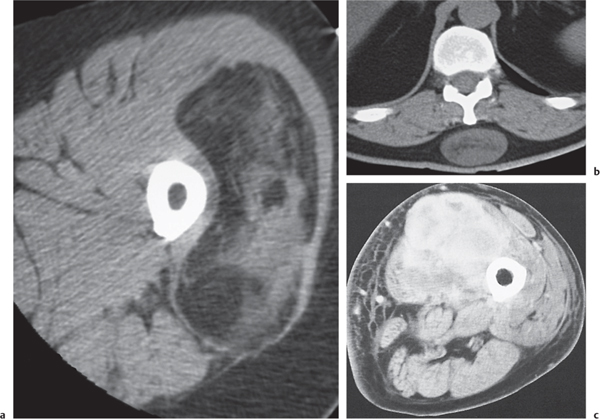
For CT, the contrast characteristics of soft tissue disease depend on the relative proportions of fat, water, and mineral. Normal muscles are of soft tissue density and are separated from each other by fatty septa. In many muscle diseases, the muscle fibers become necrotic and degenerate or are replaced by fat and connective tissue. Fatty replacement of muscle may be complete and homogeneous or incomplete and inhomogeneous, but it is not characteristic for a specific disease. It is observed with muscular dystrophies, neuropathies, ischemias, and metabolic and systemic myopathies, as well as idiopathically (Fig. 11.1). CT is of little use in the differentiation of these conditions, but it may play an important role in the localization, distribution, and assessment of the extent of muscular involvement.
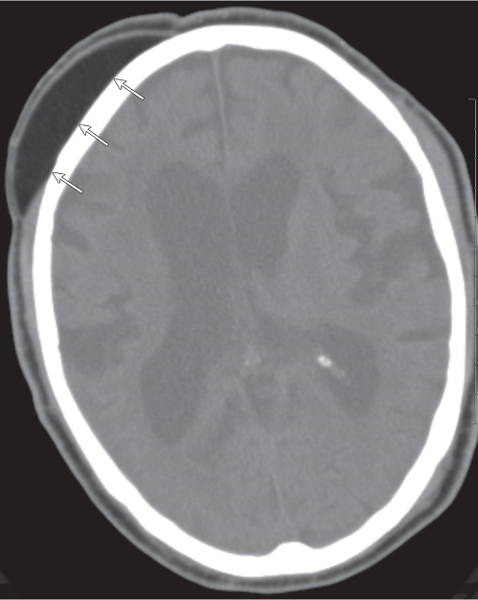
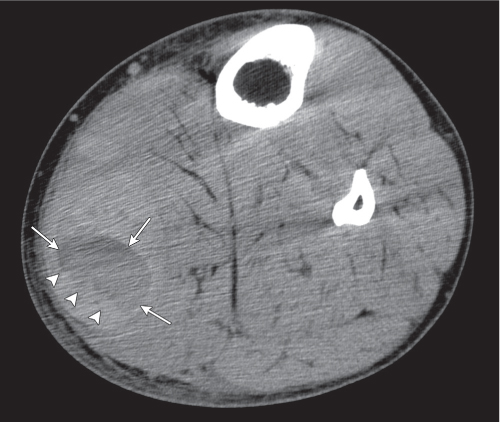
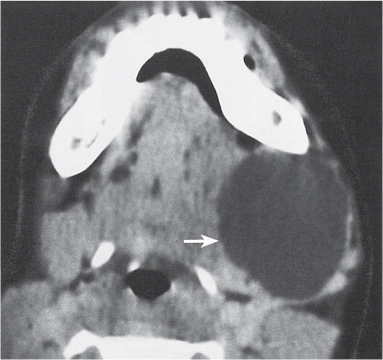
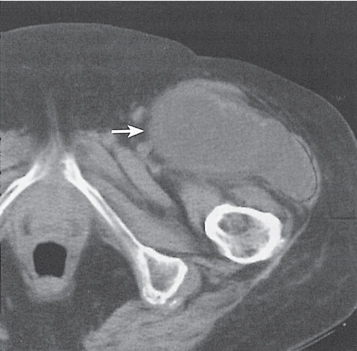
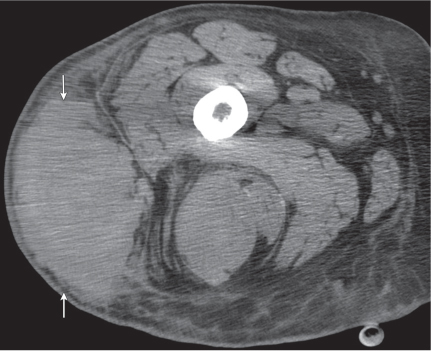
CT is useful in the evaluation of soft tissue masses. It allows definition of the exact dimensions of a lesion and its relationship to nearby neurovascular structures and bone. Certain limitations of CT in the evaluation of soft tissue masses, however, must be recognized. With the exception of a few lesions, such as lipomas (Fig. 11.2) and cysts (Fig. 11.3), CT rarely allows a specific histologic diagnosis based on attenuation values and appearance. Besides lipomas and cysts, other lesions may contain adipose tissue or fluid, respectively. The density of fat ranges from − 50 to − 100 HU. A fluid-containing lesion appears hypodense to muscle and has a density similar to water or slightly above it (range 0–20 HU). Fat-containing lesions are summarized in Table 11.1 and cystic lesions in Table 11.2.
Fig. 11.1 Muscular dystrophy. Complete fatty replacement of all muscles in the thigh is seen.Fig. 11.2 Lipoma. A fatty lesion (arrows) between the scalp and skull is seen.Fig. 11.3 Baker (popliteal) cyst. A fluid-containing lesion (arrows) hypodense to the surrounding muscles is seen. The poorly defined border on the posteroinferior border (arrowheads) indicates that the cyst is ruptured.
Table 11.1 Fat-containing soft tissue lesions
Lipoma (subcutaneous, intermuscular, intramuscular, and synovial)
Lipoma arborescens (diffuse synovial lipoma in the knee)
Neural fibrolipoma (fibrolipomatous hamartoma usually of the median nerve in the wrist)
Macrodystrophia lipomatosa (neural fibrolipoma with macrodactyly)
Lipoblastoma (lipoma in infancy and early childhood)
Hibernoma (brown fat tumor, typically involving the shoulder region, chest wall, or thigh)
Hemangioma
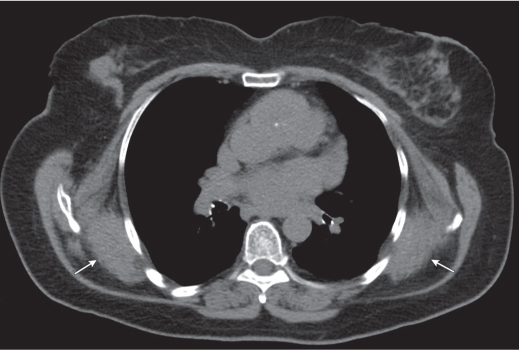
Elastofibroma (between the inferior margin of the scapula and chest wall)
Liposarcoma
Overestimation of a soft tissue mass with CT is possible because of adjacent soft tissue edema. Differentiation of actual invasion of neighboring structures such as the neurovascular bundle and bone from simple distortion and pressure defects by the adjacent mass is not always feasible.
Soft tissue calcifications can easily be appreciated by CT. They can be classified as metabolic (metastatic), dystrophic, or idiopathic.
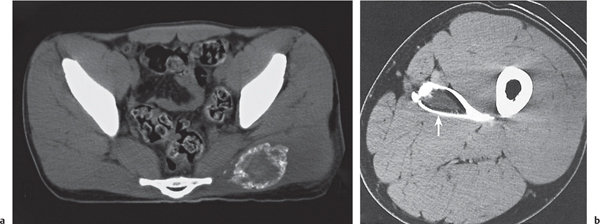
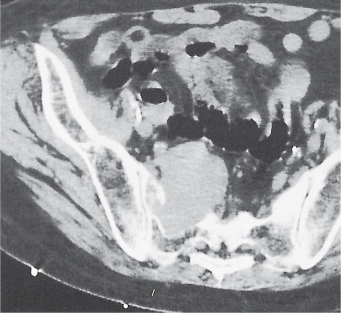
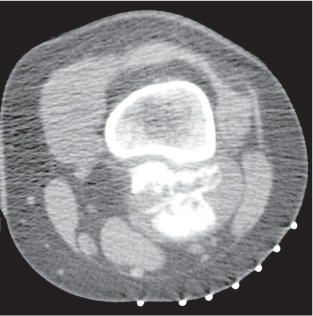
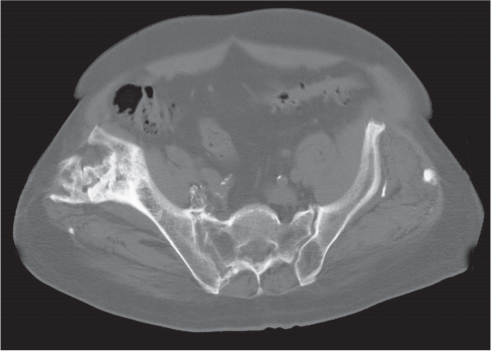
Metabolic (metastatic) calcifications are associated with a disturbance in calcium/phosphorous metabolism, resulting in the deposition of calcium in normal tissues (Fig. 11.4). Such conditions include renal osteodystrophy (less commonly, primary hyperparathyroidism), hypoparathyroidism, hypervitaminosis D, milk–alkali syndrome (prolonged excessive intake of milk and alkali for heartburn in peptic ulcer disease, often associated with renal insufficiency), sarcoidosis, and processes associated with massive bone destruction (e.g., metastases, multiple myeloma, and leukemia).
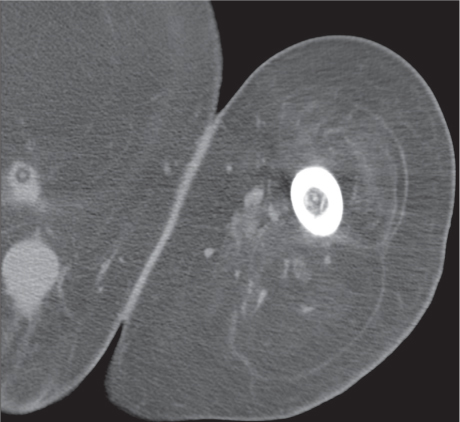
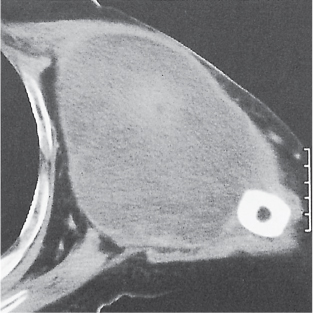
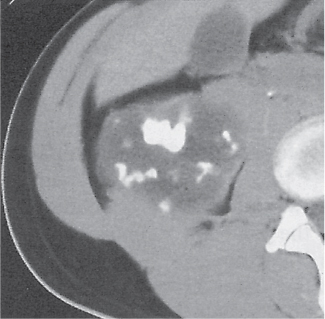
Dystrophic calcifications represent calcium deposits in damaged tissue without metabolic derangement. They are associated with traumatic, ischemic, neuropathic, infectious, and neoplastic conditions. Besides calcification of a hematoma, other traumatic causes include sequelae of previous surgery, irradiation, and thermal injuries. Foreign body and injection granulomas also frequently calcify. Subcutaneous fat necrosis resulting in calcification of the subcutaneous adipose tissue is found with pancreatic disorders, Weber–Christian disease (nonsuppurative nodular panniculitis with subsequent necrosis and fibrosis in the subcutaneous fat and all visceral adipose tissues), and vascular insufficiency, in which calcified varicose veins or arteriosclerotic arteries are frequently also present. In the infectious group, calcified abscesses and granulomas are encountered. Soft tissue calcifications are also found in a variety of parasitic infestations, such as cysticercosis and echinococcosis. Tumor calcifications occur in both benign and malignant neoplasms. In benign tumors, the calcifications may be central (e.g., in lipomas [Fig. 11.5] and hemangiomas) or peripheral (e.g., in myxomas and xanthomas). In malignant neoplasms, such as synovial sarcoma, and less commonly in other soft tissue sarcomas, such as malignant fibrous histiocytoma, leiomyosarcoma, and rhabdomyosarcoma, both necrosis and hemorrhage may lead to secondary calcifications. Extraskeletal chondrosarcomas and osteosarcomas may demonstrate irregular, poorly marginated calcific deposits, whereas calcifications in their benign counterparts (chondromas and osteomas) tend to be well defined.
Table 11.2 Cystic soft tissue lesions
Synovial cyst (cystic lesion lined by synovial membrane that may or may not communicate with the neighboring joint)
Ganglion or ganglionic cyst (arising from tendon sheaths, tendon, and muscles)
Meniscal (parameniscal) cyst (associated with chronic meniscal tears) Labral (paralabral) cyst (associated with glenoid and acetabular labral tears)
Distended bursa (commonly associated with chronic mechanical irritation, trauma, rheumatoid arthritis, and gout)
Cystic lymphangioma or hygroma (may be associated with Turner or Noonan syndrome and several trisomies)
Branchial cleft cyst (limited to the head and neck area)
Myxoma (benign subcutaneous or intramuscular cystic neoplasm, either thin-walled or thick-walled, sometimes with septation)
Chronic (liquefied) hematoma (pseudocapsule and “hematocrit effect” caused by settling of cellular elements at the bottom of the cystic lesion may occasionally be observed)
Abscess (irregular, thick-walled or, less commonly, thin-walled cystic lesion with considerable wall enhancement and surrounding edema)
Necrotic tumor (irregular, thick-walled, usually malignant)
Aneurysm and pseudoaneurysm (most common in popliteal artery)
Fig. 11.4 Renal failure. Paraspinal soft tissue calcifications are seen.Fig. 11.5 Lipoma. A fatty intramuscular lesion with central calcification is seen.Fig. 11.6 Scleroderma. Irregular calcifications about the trochanter are seen.
Phleboliths are dystrophic calcifications in organizing thrombi. They present as circular or elliptical calcifications with radiolucent centers measuring < 1 cm in their longest diameter. They are commonly found in hemangiomas and varicosities. They are quite characteristic but may occasionally be simulated by extra-articular (tenosynovial) chondromatosis, cysticercosis, and the calcified fatty deposits in Ehlers–Danlos syndrome (connective tissue disease with joint hyperextensibility and multiple musculoskeletal and other anomalies).
Idiopathic soft tissue calcifications are limited to the con nective tissue disorders (e.g., scleroderma [Fig. 11.6 ], dermatomyositis, and occasionally systemic lupus erythematosus) and idiopathic calcinosis (Fig. 11.7). In the latter conditions, the calcifications may be widespread and arranged in longitudinal bands (calcinosis universalis) or in multiple, well-demarcated masses of calcium often about articulations (tumoral calcinosis), or they may be localized (circumscript calcinosis, or calcinosis circumscripta). In tumoral and circumscript calcinosis, calcium–fluid levels are sometimes observed. Soft tissue calcifications are summarized in Table 11.3; Table 11.4 lists soft tissue calcifications commonly found in para-articular distribution.
Fig. 11.7 Tumoral calcinosis. A large calcified soft tissue mass is seen in the right thigh.
Table 11.3 Soft tissue calcifications
Metabolic (metastatic) calcifications
Hyperparathyroidism (primary; more commonly secondary, due to chronic renal disease; and, rarely, ectopic, caused by lung or kidney tumors)
Hypoparathyroidism
Hypervitaminosis D
Williams syndrome (idiopathic hypercalcemia of infancy)
Milk–alkali syndrome
Sarcoidosis
Conditions associated with massive bone destruction
(e.g., metastases, multiple myeloma, and leukemia)
Vascular disorders* (atherosclerosis, Mönckeberg sclerosis, and diabetes mellitus)
Phleboliths
Neurologic disorders*
Tumors* (synovial sarcoma, lipoma, hemangioma, cartilaginous and osteoblastic tumors, and necrotic tumors)
Infection and infestation
* Indicates that condition may progress to ossification.
(abscess, granuloma, tuberculosis, leprosy, cysticercosis, echinococcosis, dracunculiasis, and loiasis) Articular/para-articular disorders (calcific tendinosis and bursitis, gout) (see also Table 11.4)
Idiopathic calcifications
Connective tissue disorders (scleroderma, dermatomyositis, and systemic lupus erythematosus)
Calcinosis (universalis, tumoralis, and circumscripta)
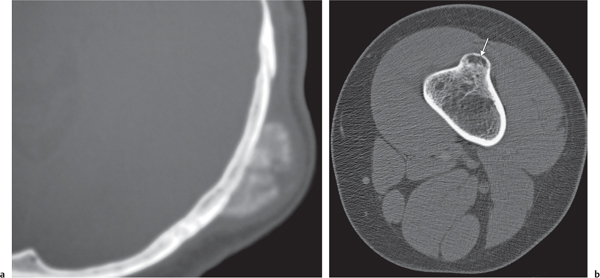
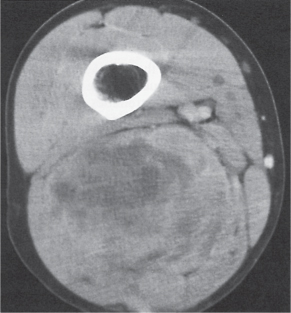
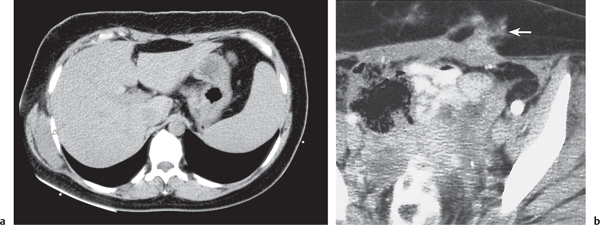
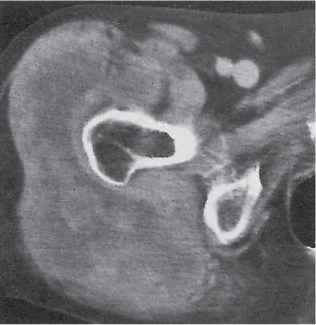
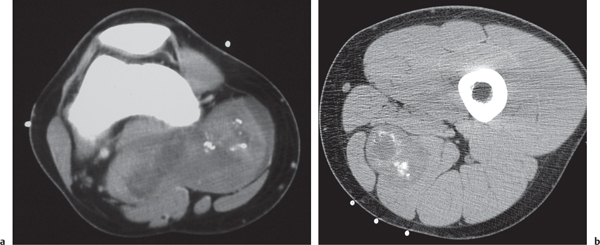
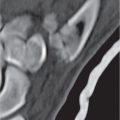
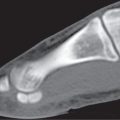
Soft tissue ossification is diagnosed when cancellous bone is surrounded by cortical bone. Because only a limited number of diseases presenting initially with soft tissue calcification may eventually progress to soft tissue ossification, the differential diagnosis of the latter is accordingly smaller. A common cause of soft tissue ossification is traumatic myositis ossificans. It is characterized by a peripheral ring of ossification (“eggshell” calcification) surrounding a more lucent center (Fig. 11.8). Furthermore, the lesion is typically separated in its entire length from the adjacent cortex when located near a bone. In the absence of a history of trauma, the same lesion is often referred to as a pseudomalignant osseous tumor of soft tissue. A parosteal osteosarcoma presents as a radiodense lesion attached in a sessile fashion to the external cortex (Fig. 11.9a). In contrast to myositis ossificans, ossification of the tumor proceeds from the base of the lesion to its periphery. An osteochondroma is composed of a medullary cavity that is contiguous with the bone from which it arose and is surrounded by sharply defined cortical bone and a thin cartilaginous cap with varying degrees of calcifications (Fig. 11.9b). Soft tissue ossifications with a predilection for the para-articular regions are found in melorheostosis, a condition in which the bony alterations are diagnostic. Heterotopic bone formation occurs commonly after surgery, especially after insertion of hip prostheses and in a variety of neurologic disorders, especially paraplegia. Venous insufficiency and thermal injuries may lead to soft tissue ossification in the extremities. Myositis ossificans progressiva (fibrodysplasia ossificans progressiva) is a rare cause of soft tissue ossification associated with anomalies and hypoplasias of the great toes and thumbs, exostoses, and progressive fusion of primarily the axial skeleton. Soft tissue ossifications are summarized in Table 11.5.
Tumors (especially synovial sarcoma and soft tissue chondrosarcoma)
Fig. 11.8a, b Traumatic myositis ossificans (two cases). (a) Early stage: A ring of calcification/ossification is seen in the periphery of a hematoma in the left gluteus maximus muscle. (b) Late stage: An ossified hematoma is seen in the left thigh (arrow).
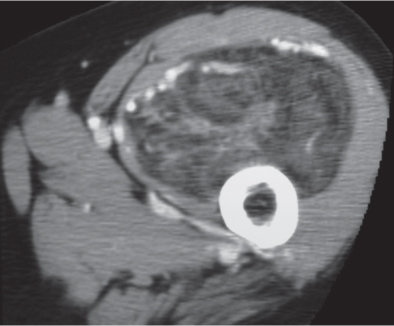
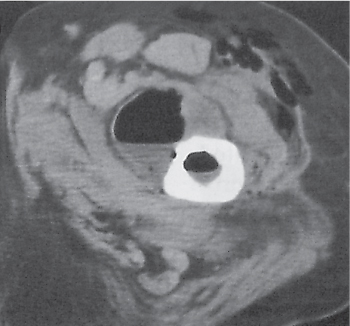
The hallmark of necrotizing fasciitis (Fig. 11.10) is the presence of soft tissue gas, but this finding is not universally present. Gas in this life-threatening condition is commonly produced by a mixture of both aerobic and anaerobic bacteria. CT features include, besides soft tissue gas, marked edematous thickening of both the superficial and deep fasciae often associated with fluid collections, whereas the edematous changes in the muscle and adipose tissue are often less severe. Cellulitis, a streptococcal or, less commonly, a staphylococcal infection, can be differentiated from necrotizing fasciitis by the predominant involvement of the subcutaneous fat and superficial fascial tissues and the absence of soft tissue gas. Pyomyositis typically affects otherwise healthy children and young adults, especially in tropical regions, but it is also recognized with increasing frequency in malnourished and immunodeficient patients. Gas bubbles are occasionally seen in this intramuscular abscess caused by a Staphylococcus aureus infection in about 90% and by a streptococcal infection in the remaining cases.
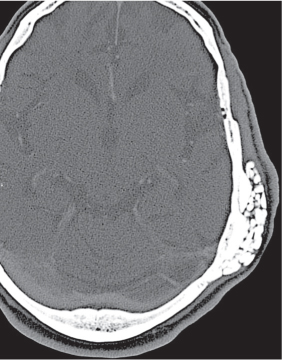
Fig. 11.9a, b Parosteal sarcoma and osteochondroma. An ossified parosteal sarcoma (a) is attached in sessile fashion to the outer table of the skull. The medullary cavity of an osteochondroma (b, arrow) is contiguous with the femur from which it arose and surrounded by sharply defined cortical bone. The cartilaginous cap without calcifications is not appreciated.
Table 11.5 Soft tissue ossification (heterotopic bone formation)
Hematoma (e.g., following total hip prosthesis)
Myositis ossificans traumatica
Myositis (fibrodysplasia) ossificans progressiva
Thermal injuries
Surgical scars
Venous insufficiency
Infection
Tumors (synovial osteochondromatosis, pseudomalignant osseous soft tissue tumor, and parosteal and extraskeletal osteosarcoma)
Melorheostosis
Neurologic disorders (paraplegia, cerebrovascular accident, poliomyelitis, and multiple sclerosis)
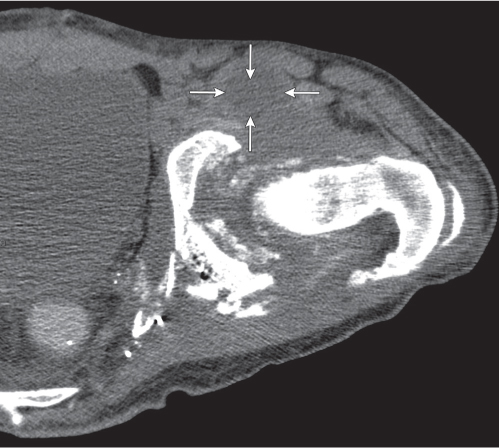
Fig. 11.10 Necrotizing fasciitis. Extensive soft tissue gas is seen in the gluteal and obturator internus muscles. The edematous changes in the adjacent subcutaneous fat are only relatively mild.
Soft tissue contamination with gas gangrene occurs in devitalized tissues in which the arterial blood supply has been compromised. Predisposing factors for this clostridial infection include contaminated wounds, burns, decubitus ulcers, and diabetes mellitus. Gas in the subcutaneous tissue presents in this condition typically as linear or netlike lucent areas, whereas in the muscles, it characteristically produces circular collections of varying sizes. Conditions associated with soft tissue gas are summarized in Table 11.6.
Differentiation between a benign and malignant soft tissue lesion is not always possible either. Features for a benign process are small size; smooth, well-defined borders; and the absence of invasion of the adjacent muscles and bones. Criteria for a malignant process include a large size, poor definition, inhomogeneous density, blurring of the adjacent fat, and invasion of the adjacent muscles and bone.
The differential diagnosis of soft tissue lesions is discussed in Table 11.7.
Table 11.6 Soft tissue gas
Skin defects (e.g., decubitus ulcer and surgical defects)
Sinus tracts and fistulas
Iatrogenic interventions
Penetrating trauma (e.g., gunshot wound)
Perforation of gas-containing structures (e.g., rib fracture with lung injury, fractured trachea)
Sharply marginated, homogeneous, unilocular or multilocular mass of water density. Higher attenuation values after intracystic hemorrhage. No enhancement after intravenous (IV) contrast administration. Occasionally, minimal enhancement of the thin cystic wall occurs.
Differential diagnosis: para-articular meniscal and labral cysts are associated with chronic tears and degeneration of the corresponding joint structures.
Cystic lesions in the vicinity of a joint usually represent a synovial cyst (herniation of the synovial membrane through the joint capsule) or a distended bursa (with or without communication with the adjacent articulation). These conditions are of traumatic, degenerative, or inflammatory origin. Rheumatoid arthritis is the most common cause of a large synovial cyst.
A ganglion (ganglion cyst) is a cystic, tumorlike lesion that is commonly attached to a tendon sheath.
A myxoma is a cystic connective soft tissue lesion, often with intratumoral septa in intramuscular, subcutaneous, or aponeurotic location.
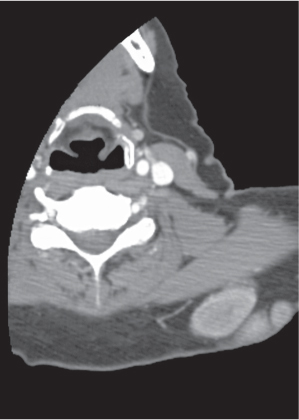
Well-defined, homogeneous, fatty soft tissue mass (−50 to −100 HU) without significant contrast enhancement is virtually diagnostic. Thin septations or vessels and calcifications or ossifications within the tumor are occasionally observed. Lipomas located close to bone (parosteal lipomas) may incite a localized hyperostosis. Invasion into the surrounding soft tissue or areas of soft tissue within the lesion suggest the possibility of a liposarcoma, although these findings might also be found with rare infiltrating varieties of lipomas and angiolipomas or with necrosis and hemorrhage occurring within a lipoma.
Most common benign soft tissue tumor. Predilection for the subcutaneous fat (superficial lipomas) in patients between 30 and 50 y of age, with female predominance. Multiple in 5% of all patients. Deep lipomas arise in the subfascial tissue or within muscle and may reach considerable size. Variants of fatty tumors include (neural) fibrolipoma, mesenchymoma (lipoma with significant chondroid and osseous metaplasia), lipomatosis (diffuse infiltrative overgrowth of mature adipose tissue), hibernoma (hypervascular tumor of brown fat usually in the shoulder region, chest wall, or thigh) (Fig. 11.16), lipoblastoma (superficial infiltrating lipomatous lesion in the extremities occurring usually in infancy and early childhood), lipoma arborescens (fatty infiltration beneath synovial joint lining, usually in the knee), and macrodystrophia lipomatosa resulting in grotesque enlargement of one or more digits in the same extremity.
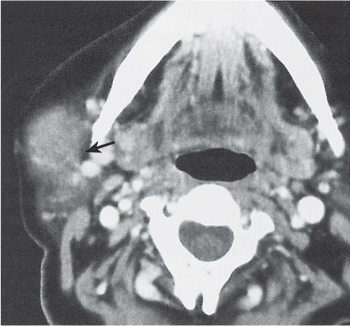
Inhomogeneous, usually relatively well-defined mass that may contain phleboliths. Hemangiomas have a density of 30 to 40 HU and enhance markedly following IV contrast medium administration. Occasionally, phleboliths are found within the lesion. When adjacent to bone, erosions and solid periosteal reactions are occasionally observed. Capillary, cavernous, venous, and arteriovenous hemangiomas are differentiated. Cavernous hemangiomas may contain a large amount of fat.
Most common vascular tumor with a predilection for the skin. Deep soft tissue hemangiomas are usually asymptomatic. Conditions associated with multiple hemangiomas include consumption coagulopathy (Kasabach–Merritt syndrome), cardiac decompensation, gangrene, massive osteolysis of Gorham, Klippel–Trenaunay syndrome (varicose veins, soft tissue and bone hypertrophy), Parkes–Weber syndrome (Klippel–Trenaunay with arteriovenous fistulas), Sturge-Weber syndrome (meningofacial angiomatosis), or Maffucci syndrome (enchondromatosis) with hemangioma.
Similar to hemangioma but without phleboliths and less contrast enhancement. Branchial cleft cysts in the head and neck area must be differentiated from a cystic lymphangioma.
Rare. Cystic lymphangioma (hygroma) may be associated with Turner and Noonan syndromes and several trisomies.
Well-defined, homogeneous lesions with marked enhancement after IV contrast administration.
Plexiform (cirsoid) neurofibromas, found only in neurofibromatosis, present as poorly circumscribed inhomogeneous lesion with potential for malignant transformation.
Solitary neurofibromas and neurilemoma (benign schwannoma, neurinoma) are slow-growing lesions found most commonly in the third to fifth decades of life.
The CT appearance of neurofibrosarcomas (Fig. 11.21) and malignant schwannomas (Fig. 11.22) is similar to their benign counterparts. They occur in approximately 50% of patients with neurofibromatosis.
Morton neuroma
Well-defined, often dumbbell-shaped lesion between metatarsal heads, frequently associated with intermetatarsal bursitis.
Fibrous response to mechanical impingement of an interdigital plantar nerve most often between the heads of the third and fourth metatarsals. Female predominance (high-heel shoes).
Unilateral or bilateral (25%), subscapular lesion of lenticular shape typically located between the inferior scapula and chest wall.
Benign, usually asymptomatic, tumorlike, fibrous lesion secondary to mechanical friction. Found in middle-aged and elderly persons with female predominance. May contain adipose tissue.
Chondroma
Well-demarcated soft tissue mass containing curvilinear, ringlike or nodular calcifications. Intracapsular chondromas arise most often in the knee.
Occurs predominantly in the third and fourth decades of life, especially in hands and feet.
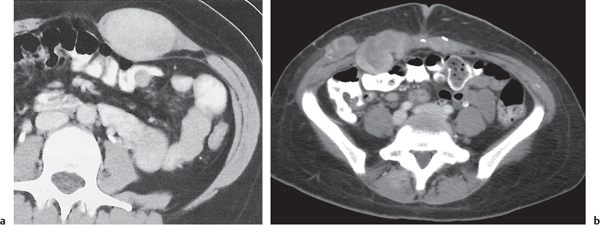
Variety of benign fibrous proliferation presenting as well or more commonly poorly defined homogeneous soft tissue lesions. May simulate a malignant lesion by infiltrating into the adjacent tissues and even bone. Recurrences are frequent.
Desmoid (Fig. 11.26a, b) arises in abdominal and extra-abdominal musculature (especially the shoulder area).
Nodular and proliferative fasciitis occurs in the extremities of adults.
Recurring digital fibromas occur in the fingers and toes of infants.
Palmar and plantar fibromatosis are fibrous proliferations of the palmar and plantar fascia.
Juvenile aponeurotic fibroma arises in the aponeurotic tissues of the hands and feet of young children. May calcify.
Congenital generalized fibromatosis occurs in infants and may affect not only soft tissues but also viscera and bone.
Well- or poorly defined, heterogeneous mass with a variable amount of fatty tissue. Because of their fibrous, myxomatous, and vascular elements, liposarcomas have a higher attenuation than lipomas and enhance with IV contrast. Calcification or ossification may be seen in well-differentiated sarcomas.
Common soft tissue malignancy of the middle-aged and elderly. Frequent involvement of the lower extremity. Histologically, five different types (well-differentiated, embryo-nal, myxoid, pleomorphic, and round cell) are recognized. With the exception of the well-differentiated liposarcoma, these neoplasms are highly malignant.
Well- or poorly defined, inhomogeneous soft tissue mass, often with necrotic (hypodense) areas and considerable contrast enhancement. Erosion/destruction of an adjacent bone occurs. A periosteal reaction is, however, rare unless a pathologic fracture has occurred. Intratumoral calcifications are unusual.
Most common primary malignant soft tissue tumor. Occurs at all ages, most often around age 50 y. Slight male predominance. Lower extremity is the most frequent location.
Fibrosarcomas have similar radiologic and histologic features but appear overall slightly less malignant.
Dermatofibrosarcoma protuberans (Fig. 11.29) presents as single or multiple nodules in the skin or subcutaneous tissue of the trunk and, less commonly, the extremities and the head and neck.
Fairly well to poorly defined soft tissue mass. Erosion or invasion of the adjacent bone common. Inhomogeneous appearance after necrosis, hemorrhage, and cystic degeneration. Leiomyosarcomas (Fig. 11.31) present in similar fashion, but large areas of tumor necrosis, which may eventually calcify, are common. These neoplasms are most often found in the retroperitoneum or thigh or may be associated with major blood vessels (e.g., saphenous vein).
Occurs usually under the age of 50 y. In adults, the tumor is usually located in the deeper tissues of the extremities and torso. In children, the tumor predominates in the head, neck, and urogenital tract.
The benign rhabdomyoma is an extremely rare tumor of benign striated muscle cells.
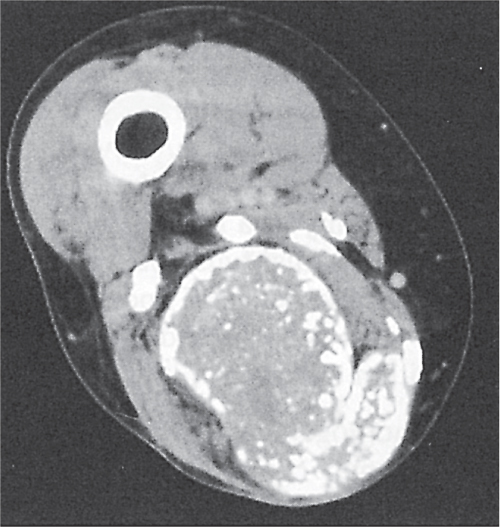
Relatively poorly defined, usually inhomogeneous mass with calcifications in 30% and erosion/destruction of adjacent bone without reactive sclerosis in 20% of cases.
Most frequently seen in the thigh and lower extremity, usually in young adults, but all ages can be affected. Calcified metastases are not uncommon, especially in the lungs, but they may be late (several years after initial diagnosis).
Well- or poorly defined mass lesions that may erode or invade the adjacent bone.
Metastases, melanomas, lymphomas, extraosseous plasmacytomas, angiosarcomas, clear cell sarcomas (also known as malignant melanomas of soft parts; arise in vicinity of tendons and aponeuroses, most commonly in the foot and ankle), alveolar soft tissue sarcomas (malignant granular cell myoblastoma) originating in muscles, epithelioid sarcomas (arising primarily in fingers, hands, and forearms of young adults), Askin tumors (neuroectodermal small cell tumors arising from intercostal nerves), and primary soft tissue osteosarcomas, Ewing sarcomas, primitive neuroectodermal tumor (PNET), and chondrosarcomas.
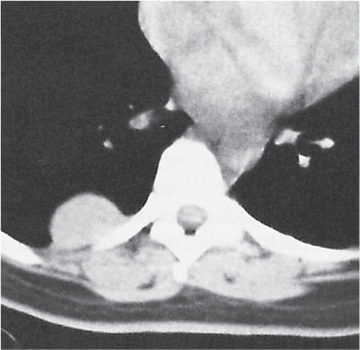
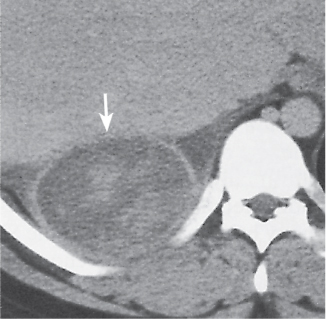
Poorly defined, isodense or slightly hypodense mass (early stage) or, more commonly, well-defined cystic lesion with a relatively thick wall and occasionally septation. The attenuation value of the liquefied content frequently exceeds 25 HU. Enhancement of the nonliquefied components after contrast administration. Presence of soft tissue gas in the absence of surgical or percutaneous intervention is rare but virtually diagnostic.
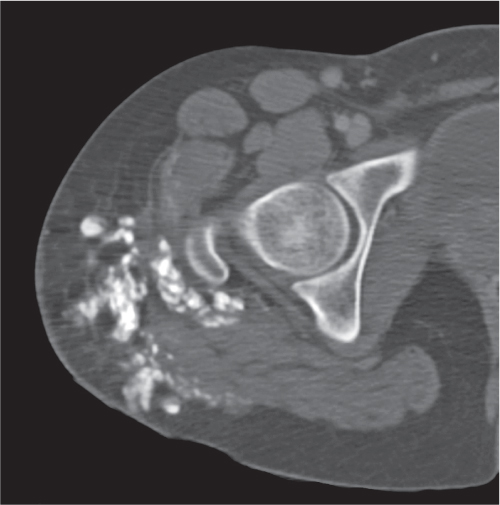
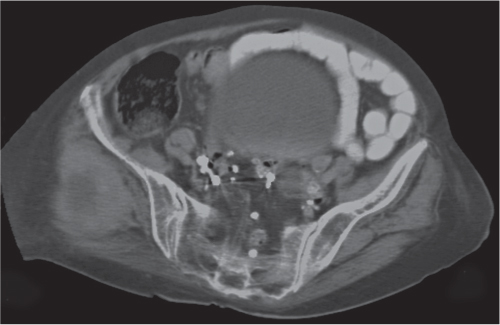
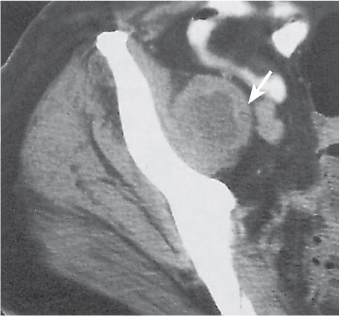
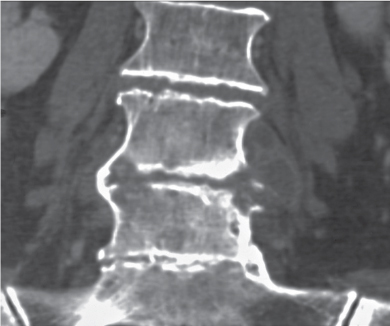
Common causes of soft tissue abscesses include penetrating traumas, iatrogenic interventions, IV drug abuse, spread from a contiguous infection, and septic embolism. In tuberculous spondylitis, a fusiform psoas abscess with amorphous or teardrop-shaped calcifications is often associated (Fig. 11.40).
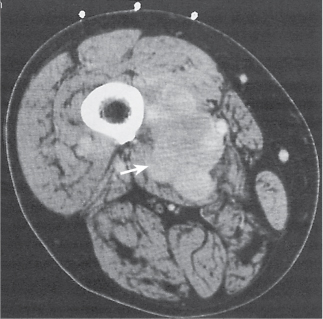
Homogeneous enlargement of the involved muscle, which might be hyperdense in the acute stage. In the subacute stage, the hematoma may be poorly defined and is either isodense or slightly hypodense. With liquefaction, it progresses to a patchy or inhomogeneous appearance. When completely liquefied, the hematoma again has a homogeneous density that is lower than muscle and may be surrounded by a pseudocapsule that enhances after contrast administration. A “hematocrit effect” caused by settling of the cellular elements within the liquefied hematoma is occasionally observed. Calcification and ossification (myositis ossificans) can occur in a later stage.
Soft tissue hemorrhage occurs spontaneously, following trauma or surgery, with a variety of bleeding disorders, and during anticoagulation therapy. Bleeding into a tumor or abscess is quite common.
Aneurysm/pseudoaneurysm
Round soft tissue density with occasionally curvilinear calcification in the vicinity of a major artery. Inhomogeneous appearance when partially thrombosed. IV contrast administration is diagnostic.
Popliteal artery aneurysm is the most common aneurysmatic lesion found in the extremities and presents as a pulsatile mass.
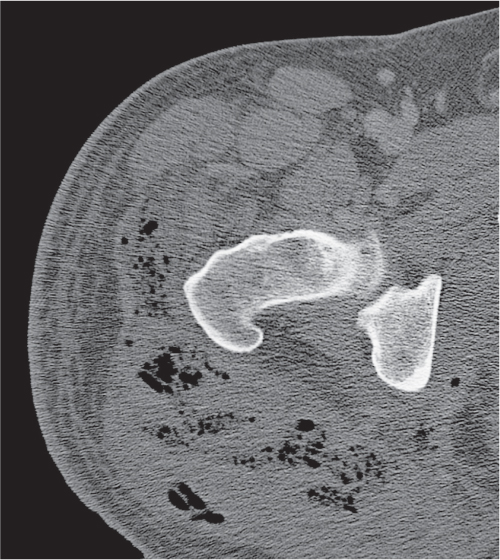
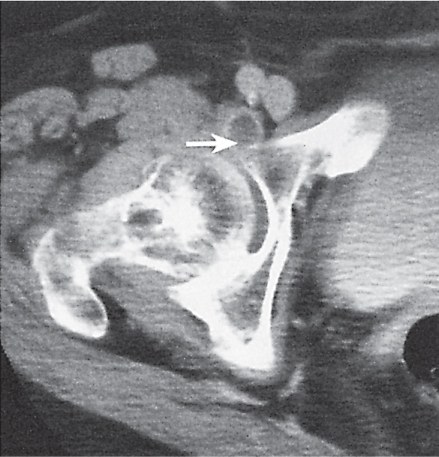
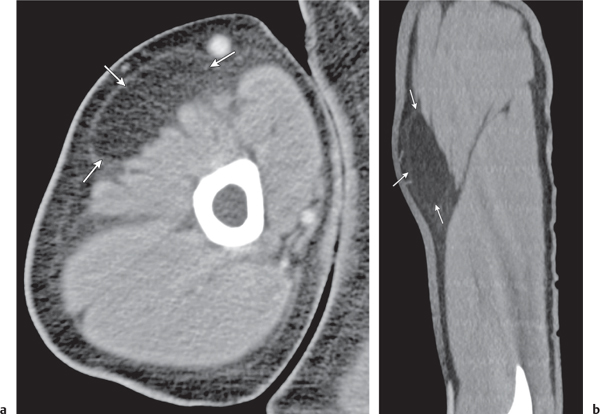
Fig. 11.11 Synovial cyst in rheumatoid arthritis. Small cyst (arrow) connecting with the right hip joint projects anterior to the acetabulum.Fig. 11.12 Iliopsoas bursitis. An enlarged iliopsoas bursa containing serous fluid is seen (arrows). An infected hemorrhagic and destroyed hip with numerous loose fracture fragments secondary to gunshot injury is also present.Fig. 11.13a, b Subcutaneous lipoma. A fatty lesion (arrows) is seen in the upper arm that is difficult to demarcate from the normal surrounding adipose tissue (a, axial; b, sagittal).Fig. 11.14 Intramuscular lipoma. A well-circumscribed fatty lesion is seen in the quadriceps femoris muscle of the thigh.Fig. 11.15 Lipoma. A fatty lesion with central calcification is seen in the lower leg.Fig. 11.16 Hibernoma. A fatty lesion containing soft tissue components is seen in the thigh. The lesion cannot be differentiated radiographically from a liposarcoma.Fig. 11.17 Hemangioma (capillary). An enhancing mass is seen in the right lateral face (arrow).Fig. 11.18 Hemangioma. Multiple calcifications (phleboliths) are seen in a scalp lesion with induction of new bone formation in the adjacent outer table of the skull.Fig. 11.19 Lymphangioma. A large cystic mass projects behind the left mandibular angle.Fig. 11.20 Schwannoma. A well-defined homogeneous mass is eroding the adjacent sacral foramen.Fig. 11.21 Neurofibrosarcoma. A well-defined, huge, hypodense soft tissue mass arising from the left armpit is seen in this patient with neurofibromatosis.Fig. 11.22 Malignant schwannoma. A relatively poorly defined mass with inhomogeneous, hypodense central areas is evident in the thigh.Fig. 11.23 Elastofibroma. Bilateral slightly inhomogeneous lesions (arrows) adjacent to the posterolateral chest wall just beneath the inferior scapular angles are seen.Fig. 11.24 Pleural fibroma (benign mesothelioma). A well-defined homogeneous mass arises from the posterior pleura.Fig. 11.25a, b Fibromatosis (two cases). A well-defined oblong soft tissue mass (a) is seen in the right posterolateral abdominal wall (arrow). A more aggressive lesion (b) is evident as a poorly defined soft tissue density in the left anterior abdominal wall (arrow).Fig. 11.26a, b Desmoid (two patients). An oval-shaped, homogeneous mass (a) is seen in the left anterior abdominal wall. Well-circumscribed, somewhat irregular outlined lesions (b) with hypodense centers are seen in the right anterior abdominal wall.Fig. 11.27a–c Liposarcoma (three different patients). A fatty mass (a) containing irregular soft tissue components is seen in the thigh. A well-circumscribed ovoid mass (b) containing only small amounts of fatty tissue in its center is seen posterior of the spine. A relatively well-defined heterogeneous mass (c) containing only a small amount of fatty tissue is seen in the anterior thigh.Fig. 11.28 Malignant fibrous histiocytoma. A relatively poorly defined homogeneous soft tissue mass is evident (arrow).Fig. 11.29 Dermatofibrosarcoma protuberans. A subcutaneous lesion with a hypodense center and adjacent nodular thickening of the skin is seen.Fig. 11.30 Rhabdomyosarcoma. A relatively well-defined inhomogeneous mass surrounds the right proximal femur.Fig. 11.31 Leiomyosarcoma. A large pear-shaped mass with a hypodense (necrotic) center is seen lateral to the right pelvis.Fig. 11.32a, b Synovial sarcoma (two cases). A poorly defined mass with multiple irregular calcifications and slightly lower attenuation than the adjacent muscles is seen posterior to the knee (a) and in the semimembranosus muscle of the thigh (b).Fig. 11.33 Alveolar soft tissue sarcoma. A lobulated, relatively well-defined soft tissue mass is seen in the thigh (arrow).Fig. 11.34 Askin tumor. A well-defined, slightly inhomogeneous mass arising from the intercostal nerve projects between the posterior chest wall and liver (arrow).Fig. 11.35 Soft tissue chondrosarcoma. A relatively well-defined soft tissue mass with scattered calcifications is seen.Fig. 11.36 Soft tissue osteosarcoma. An irregular ossified mass not attached to the distal femur is seen.Fig. 11.37 Abscesses. Thick-walled cystic lesions are seen projecting medially and laterally to the ischium in this paraplegic patient with decubitus ulcers. Note also the thick periosteal reaction along the lateral aspect of the ischium.Fig. 11.38 Abscess. The iliopsoas abscess presents a cystic lesion with an irregular thick wall (arrow).Fig. 11.39 Gas-forming abscess. A thin-walled cystic lesion with air–fluid level projects anteromedial to the left femur. A second fluid level is seen in the femur. Note also the irregular gas collections in the anterolateral soft tissues of the thigh.Fig. 11.40 Psoas abscess in tuberculous spondylitis. Disk space narrowing with erosion of the adjacent end plates most apparent at the adjacent corners of the L4–L5 vertebral bodies is seen. On the right side, the tuberculous infection is sealed offby a bridging periosteal reaction; on the left side, a tuberculous psoas abscess presenting as an oblong soft tissue mass containing loculated hypodense foci and two small calcifications is seen.Fig. 11.41 Subacute hematoma. A large subcutaneous mass (arrows) isodense to muscle is seen.Fig. 11.42 Traumatic myositis ossificans. A healing right iliac crest fracture with extensive surrounding heterotopic bone formation is seen.
Only gold members can continue reading. Log In or Register to continue