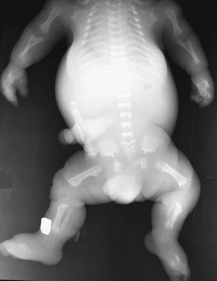
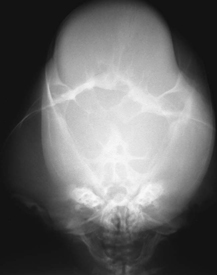
CASE 113 Two stillborn term infants present with similar short-limbed dwarfism. Figure 113A Figure 113B Figure 113C The stillborn neonate in Fig. 113A demonstrates dramatic platyspondyly with markedly shortened ribs and severe micromelia with markedly curved humeri and femora, with the latter showing characteristic “telephone receiver” appearance. Marked shortening of digits and metacarpals (brachy-dactyly and brachymetacarpalia) of hands is noted without evidence of craniosynostosis. The stillborn neonate in Figs. 113B and 113C shows dramatic platyspondyly with markedly shortened ribs, severe micromelia with straight long bones, marked brachydactyly and brachymetacarpalia, and “cloverleaf” or kleebattschädel skull, indicative of universal craniosynostosis. Thanatophoric dysplasia (TD), type 1 (Fig. 113A) and type 2 (Figs. 113B and 113C) Although many skeletal dysplasias are compatible with a normal life span, lethal dysplasias do exist. Aside, perhaps, from type 2 osteogenesis imperfecta, the most common lethal skeletal dysplasia is TD. The term thanatophoric is from the Greek, meaning “death bearing.” Most patients are stillborn, with the vast majority of affected live-born neonates succumbing within the first week. It is important to accurately diagnose the lethal skeletal dysplasias in order to tailor supportive care and to counsel parents regarding the relative risk for recurrence in subsequent pregnancies. TD occurs as two major, distinct subtypes, with several additional “thanatophoric variants” also recognized. Classic TD occurs in 1 in 35,000 to 1 in 50,000 births. TD type 1 (TD1) is characterized by severe micromelia, with curved long bones (especially the femora) having a “telephone receiver” appearance. Craniosynostosis is seen in 27.6% of patients with TD1, and it is mild in many cases. TD type 2 (TD2) is characterized by relatively straight but short long bones; however, craniosynostosis is almost universal (>93%) and is severe, resulting in a cloverleaf appearance of the calvarium (kleebattschädel) in 53%.
Clinical Presentation

Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Etiology
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


