CASE 121 Stillborn with a small chest and mild limb shortening Figure 121A Figure 121B Figure 121C Anteroposterior (Fig. 121A) and lateral (Fig. 121B) chest radiographs demonstrate severe shortening of the ribs, with a resultant small thoracic cavity. The iliac wings are small and squared, with flattened acetabular roofs, narrow sacrosciatic notches, and prominent spikes at the medial and lateral acetabular margins. Proximal femoral metaphyses are irregular. There is mild limb shortening. The clavicles demonstrate a “handlebar” appearance. The hands (Figs. 121C1 and 121C2) and feet (Fig. 121C3) demonstrate mild shortening of metatcarpals, metatarsals, and phalanges. Asphyxiating thoracic dystrophy (ATD); Jeune syndrome Several skeletal dysplasias manifest with respiratory insufficiency, small thoracic cavity, and shortening of ribs. The most common of these entities is ATD (Jeune syndrome), a fairly uncommon autosomal recessive condition first described in 1955 by Jeune, that demonstrates a spectrum of clinical severity. Severely affected newborns may die of respiratory insufficiency, whereas patients who survive the neonatal period often develop renal insufficiency later in life due to a concomitant cystic renal dysplasia. The incidence of ATD is 1 in 100,000 to 130,000 live births.
Clinical Presentation
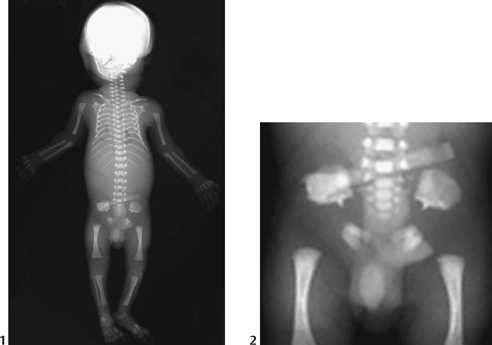

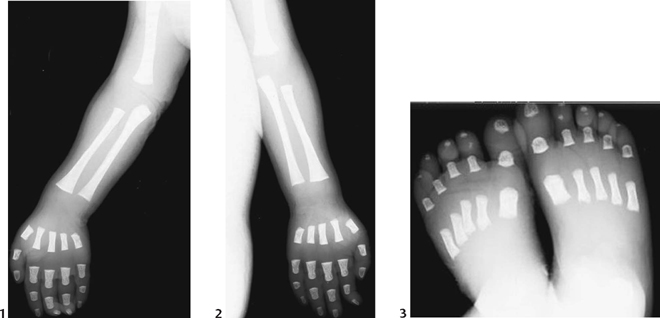
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Etiology
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


