CASE 130 A 28-year-old woman presents with pelvic pain and dyspareunia. Fig. 130.1 (A–C) Axial, sagittal, and coronal T2-weighted images of the pelvis show a well-defined T2 hyperintense lesion (arrows) located within the wall of the left vaginal fornix. (D) T1-weighted axial image after intravenous gadolinium administration shows mild peripheral rim enhancement in the lesion (arrow). Axial, sagittal, and coronal T2-weighted images of the pelvis (Fig. 130.1A,B,C) show a well-defined T2 hyperintense lesion located within the wall of the left vaginal fornix; after intravenous gadolinium administration, the lesion shows mild peripheral rim enhancement (Fig. 130.1D). Gartner duct cyst Gartner duct cysts derive from the vestigial remnant of the vaginal portion of the mesonephric (wolffian) duct; in the case of incomplete involution, cysts may develop due to secretion by persistent glandular tissue. Remnants of the mesonephric duct may be found in one fourth of women, although the cysts are rarely described (1–2%). Gartner cysts are typically paravaginal and located within the anterolateral aspect of the proximal third of the vagina.
Clinical Presentation
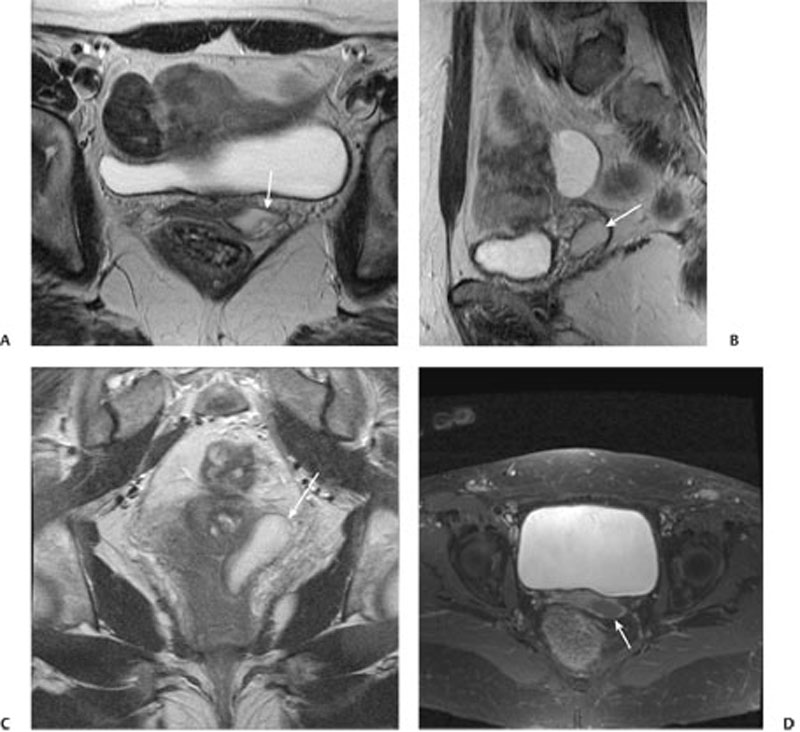
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Clinical Findings
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


