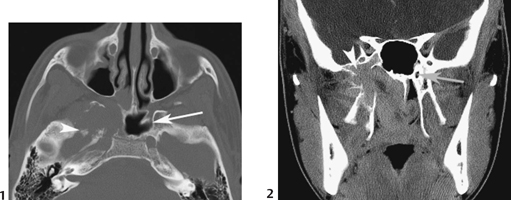
CASE 18 A 16-year-old adolescent male presents with right-sided nasal obstruction and epistaxis. Figure 18A Axial CT, soft tissue (Fig. 18A1) and bone (Fig. 18A2) windows, at the level of the maxillary sinus show characteristic features of juvenile nasopharyngeal angiofibroma. There is an enhancing mass expanding and extending into the posterior nasal air space with erosion of the base of the right pterygoid plate and lateral extension to the infratemporal fossa. Juvenile nasopharyngeal angiofibroma Juvenile angiofibroma is the most common benign nasopharyngeal tumor; nevertheless, it is uncommon and accounts for only 0.05% of all head and neck neoplasms. An incidence of 1:5000 to 1:60,000 in otolaryngology patients has been reported. This tumor was described by Hippocrates, but the term angiofibroma was first used by Friedberg in 1940 to describe this fibrovascular tumor. It occurs almost exclusively in prepubertal and adolescent males. The age range is 7 to 20 years, median 15 years, and hence the lesion is referred to frequently as juvenile angiofibroma. The male gender predilection is so typical that some authors suggest chromosomal analysis in the rare instance it occurs in females. This is a highly vascular tumor, and severe bleeding may accompany biopsy. For this reason, surgeons are reluctant to undertake biopsy of a nasopharyngeal mass in an adolescent male patient and prefer to rely on imaging methods for deciding whether the mass is likely to be an angiofibroma or a nonvascular lesion such as an antrochoanal polyp. Different staging systems exist for nasopharyngeal angiofibroma. The two most commonly used systems for treatment planning and prognosis are those of Sessions and of Fisch. The vast majority of angiofibromas originate from the pterygopalatine fossa in the recess behind the sphenopalatine ganglion at the anterior aperture of the pterygoid canal (Lloyd et al, 1999). Figure 18B Axial (1) and coronal (2) CT show an enhancing mass invading and expanding the base of the right pterygoid process. There is extension along the line of the pterygoid canal (normal contralateral side indicated by arrow) with invasion of the greater wing of the sphenoid sinus (arrowhead). There is involvement of the right lateral wall of the sphenoid sinus. The mass extends into the nasal cavity, crossing the midline to involve the contralateral side. The cause of this tumor remains unclear. Suggested theories include a hormonal theory due to the lesion’s occurrence in adolescent males; a desmoplastic response of the nasopharyngeal periosteum or the embryonic fibrocartilage between the basiocciput and the basisphenoid; and origin from nonchromaffin paraganglionic cells of the terminal branches of the maxillary artery. Symptoms of angiofibromas are numerous and nonspecific. Epistaxis (either severe or blood stained, mostly unilateral and recurrent) and nasal obstruction are the most common symptoms. There must be a high index of suspicion of this neoplasm in any prepubertal or adolescent male with a nasal mass lesion and either of these two symptoms. Other symptoms include:
Clinical Presentation
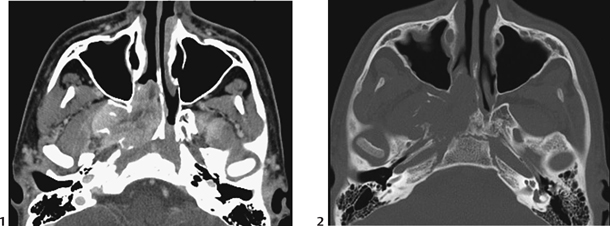
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Staging Systems
Etiology
Clinical Findings
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


