Mild ventricular enlargement can occur without associated cerebral or cerebellar abnormality.
Ventricular size usually increases with age, most pronounced after age 60 y.
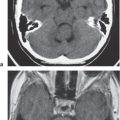
Aqueductal stenosis
Dilation of lateral and third ventricles with normalsized fourth ventricle, with or without dilation of only the upper portion of cerebral aqueduct and not the lower portion, with or without discrete or poorly defined lesion in midbrain.
Aqueductal stenosis can result from a small lesion/neoplasm in the midbrain, debris or adhesions from hemorrhage, or inflammatory diseases. CT and MRI can exclude other lesions, causing obstruction of CSF flow through the aqueduct, such as lesions in the posterior third ventricle or posterior cranial fossa.
Chiari I malformation
Cerebellar tonsils extend > 5 mm below the foramen magnum in adults, 6 mm in children younger than 10 y. Syringohydromyelia in 20% to 40%, hydrocephalus in 25%. Basilar impression in 25%. Less common association: Klippel-Feil syndrome; atlanto-occipital assimilation.
Cerebellar tonsillar ectopia. Most common anomaly of central nervous system (CNS). Not associated with myelomeningocele.
Chiari II malformation (Arnold-Chiari malformation)
Small posterior cranial fossa with gaping foramen magnum through which there is an inferiorly positioned vermis associated with a cervicomedullary kink. Beaked dorsal margin of the tectal plate. Myelomeningoceles in nearly all patients. Hydro-cephalus and syringomyelia common. Dilated lateral ventricles posteriorly (colpocephaly).
Complex anomaly involving the cerebrum, cerebellum, brainstem, spinal cord, ventricles, skull, and dura. Failure of fetal neural tube to develop properly, resulting in altered development affecting multiple sites of the CNS.
Chiari III malformation
Features of Chiari II plus lower occipital or high cervical encephalocele.
Vermian aplasia or severe hypoplasia, communication of fourth ventricle with retrocerebellar cyst, enlarged posterior fossa, high position of tentorium, and transverse venous sinuses. Hydrocephalus common. Associated with other anomalies, such as dysgenesis of the corpus callosum, gray matter heterotopia, schizencephaly, holoprosencephaly, and cephaloceles.
Abnormal formation of the roof of the fourth ventricle with absent or near incomplete formation of the cerebellar vermis.
Dandy-Walker variant
Mild vermian hypoplasia with communication of the posteroinferior portion of the fourth ventricle with the cisterna magna. No associated enlargement of the posterior cranial fossa.
Occasionally associated with hydrocephalus, dysgenesis of the corpus callosum, gray matter heterotopia, and other anomalies.
Asymmetric enlargement of the occipital horns of the lateral ventricles.
Associated with Chiari II malformations and dysgenesis of the corpus callosum.
Neoplasms (causing obstructive hydrocephalus)
Metastatic tumor
Single or multiple well-circumscribed or poorly defined lesions involving the brain, skull, dura, leptomeninges, ventricles, choroid plexus, or pituitary gland; low to intermediate attenuation; usually with contrast enhancement, with or without bone destruction, with or without compression of neural tissue or vessels. Leptomeningeal tumor often best seen on postcontrast images.
Metastatic tumor may have variable destructive or infiltrative changes involving single or multiple sites of involvement.
Intra-axial primary tumors
Astrocytoma
Low-grade astrocytoma: Focal or diffuse mass lesion usually located in the cerebellar white matter or brainstem with low to intermediate attenuation, with or without mild contrast enhancement. Minimal associated mass effect.
Often occurs in children and adults (age 20–40 y). Tumors comprised of well-differentiated astrocytes. Association with neurofibromatosis type 1; 10-y survival; may become malignant.
Juvenile pilocytic astrocytoma-subtype: Solid/cystic focal lesion with low to intermediate attenuation, usually with prominent contrast enhancement. Lesions located in cerebellum and brainstem.
Common in children; usually favorable prognosis if totally resected.
Gliomatosis cerebri: Infiltrative lesion with poorly defined margins with mass effect located in the white matter, with low to intermediate attenuation; usually no contrast enhancement until late in disease.
Diffusely infiltrating astrocytoma with relative preservation of underlying brain architecture. Imaging appearance may be more prognostic than histologic grade; ~2-y survival.
Anaplastic astrocytoma: Often irregularly marginated lesion located in the white matter with low to intermediate attenuation, with or without contrast enhancement.
Intermediate between low-grade astrocytoma and glioblastoma multiforme; ~2-y survival.
Giant cell astrocytoma (tuberous sclerosis)
Circumscribed lesion located near the foramen of Monro with mixed low to intermediate attenuation, with or without cysts and/or calcifications, with heterogeneous contrast enhancement.
Subependymal hamartoma near the foramen of Monro; occurs in 15% of patients with tuberous sclerosis younger than 20 y; slow-growing lesions can progressively cause obstruction of CSF flow through the foramen of Monro; long-term survival usual if resected.
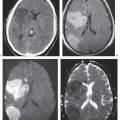
Medulloblastoma (primitive neuroectodermal tumor of the cerebellum)
Circumscribed or invasive lesions, low to intermediate and/or slightly high; variable contrast enhancement; frequent dissemination into the leptomeninges.
Highly malignant tumors that frequently disseminate along CSF pathways.
Ependymoma
Circumscribed spheroid or lobulated infratentorial lesion, usually in the fourth ventricle, with or without cysts and/or calcifications; low to intermediate attenuation, variable contrast enhancement, with or without extension through the foramina of Luschka and Magendie.
Occurs more commonly in children than adults; two thirds infratentorial, one third supratentorial.
Hemangioblastoma
Circumscribed tumors usually located in the cerebellum and/or brainstem; small contrast-enhancing nodule with or without cyst, or larger lesion with prominent heterogeneous enhancement with or without vessels within lesion or at the periphery; occasionally lesions have evidence of recent or remote hemorrhage.
Multiple lesions occur in adolescents with von HippelLindau disease.
Circumscribed and/or lobulated lesions with papillary projections, intermediate attenuation, usually prominent contrast enhancement, with or without calcifications. Locations: atrium of lateral ventricle (children) > fourth ventricle (adults), rarely other locations such as third ventricle; associated with hydrocephalus.
Rare intracranial neoplasms, CT and MRI features of choroid plexus carcinoma and papilloma overlap; both histologic types can disseminate along CSF pathways and invade brain tissue.
Meningioma
Well-circumscribed intraventricular lesions; intermediate attenuation; usually prominent contrast enhancement, with or without calcifications.
Usually benign neoplasms; typically occurs in adults (> 40 y), women > men. Multiple meningiomas seen with neurofibromatosis type 2; can result in compression of adjacent brain parenchyma, encasement of arteries, and compression of dural venous sinuses; hydrocephalus; rarely invasive/malignant types.
Hemangiopericytoma
Extra-axial mass lesions, often well circumscribed; intermediate attenuation, prominent contrast enhancement (may resemble meningiomas); with or without associated erosive bone changes.
Rare neoplasms in young adults (males > females) sometimes referred to as angioblastic meningioma or meningeal hemangiopericytoma; arise from vascular cells/pericytes; frequency of metastases > meningiomas.
Central neurocytoma
Circumscribed lesion located at margin of lateral ventricle or septum pellucidum with intraventricular protrusion, heterogeneous intermediate attenuation, with or without calcifications and/or small cysts; heterogeneous contrast enhancement.
Rare tumors that have neuronal differentiation; imaging appearance similar to intraventricular oligodendrogliomas; occur in young adults; benign slow-growing lesions.
Atypical teratoid rhabdoid tumors
Circumscribed mass lesions with intermediate attenuation, with or without zones of hemorrhage, cysts, calcifications; usually prominent contrast enhancement with or without heterogeneous pattern.
Rare malignant tumors involving the CNS usually occurring in the first decade. Histologically appear as solid tumors with or without necrotic areas, similar to malignant rhabdoid tumors of the kidney. Associated with CSF tumor dissemination and poor prognosis.
Intraventricular lesions
Colloid cyst
Well-circumscribed spheroid lesions located at the anterior portion of the third ventricle; variable attenuation (low, intermediate, or high); no contrast enhancement.
Benign epithelial-lined cyst; common presentation of headaches and intermittent hydrocephalus; removal leads to cure.
Neuroepithelial cyst
Well-circumscribed cysts with low attenuation, thin walls; no contrast enhancement or peripheral edema.
Cyst walls have histopathologic features similar to epithelium; neuroepithelial cysts located in choroid plexus > choroidal fissure > ventricles > brain parenchyma.
Curvilinear and/or nodular gadolinium enhancement along ventricular/ependymal margins with resultant communicating or noncommunicating types of hydrocephalus.
Complications of intracranial inflammatory processes, such as infections from bacteria, fungi, tuberculosis, viruses (cytomegalovirus [CMV]), and parasites. Noninfectious diseases such as sarcoid can result in a similar pattern.
Cysticercosis
Single or multiple cystic lesions in brain or meninges.
Acute/subacute phase: low to intermediate attenuation; rim with or without nodular pattern of contrast enhancement, with or without peripheral edema.
Chronic phase: Calcified granulomas.
Caused by ingestion of ova (Taenia solium) in contaminated food (undercooked pork); involves meninges > brain parenchyma > ventricles.
Hydatid cyst
Echinococcus granulosus: Single or rarely multiple cystic lesions with low attenuation, thin walls; typically no contrast enhancement or peripheral edema unless superinfected; often located in vascular territory of the middle cerebral artery.
Echinococcus multilocularis: Cystic (with or without multilocular) and/or solid lesions; central zone of intermediate attenuation surrounded by a slightly thickened rim, with contrast enhancement; peripheral zone of edema and calcifications are common.
Caused by parasites E. granulosus (South America, Middle East, Australia, and New Zealand) and E. multilocularis (North America, Europe, Turkey, and China). CNS involvement in 2% of cases of hydatid infestation.
Rasmussen encephalitis
Progressive atrophy of one cerebral hemisphere involving the white matter, basal ganglia, and cortex, usually without enhancement; ipsilateral dilated lateral ventricle.
Usually seen in children younger than 10 y; severe and progressive epilepsy and unilateral neurologic deficits: hemiplegia, psychomotor deterioration, chronic slow viral infectious process possibly caused by CMV or Epstein-Barr virus. Treatment: hemispherectomy.
Intraventricular hemorrhage from trauma, aneurysm, arteriovenous malformation (AVM), or extension of intra-axial hematoma can result in acute and/or chronic dilation of the ventricles.
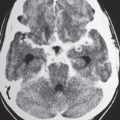
Hydranencephaly
Replacement of substantial portions of cerebral tissue with thin-walled sacs containing CSF; inferomedial portions of frontal and temporal lobes often preserved; cerebellum and thalami usually have a normal appearance.
In utero destruction of cerebral parenchyma from injury (vascular or infectious, e.g., CMV and toxoplasmosis). Patients may be normo-, micro-, or macrocephalic. Children developmentally delayed.
Irregular, relatively well-circumscribed zone with low attenuation similar to CSF, surrounded by poorly defined thin zone of decreased attenuation in adjacent brain tissue; no contrast enhancement or peripheral edema.
Represents remote sites of brain injury (trauma, infarction, infection, or hemorrhage) occurring in late second trimester with evolution by an encephaloclastic process into a cystic zone with CSF. MRI signal characteristics surrounded by zones of gliosis in adjacent brain parenchyma. Gliosis (high T2 signal) allows differentiation from schizencephaly.
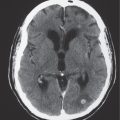
Poorly defined zone of decreased attenuation in brain tissue (gray and or white matter) with localized volume loss and compensatory dilation of adjacent ventricle.
Damaged residual brain tissue characterized by astrocytic proliferation related to prior infarct, hemorrhage, inflammation, infection, and trauma, with compensatory ipsilateral ventricular dilation resulting from localized volume loss.
Encephalomalacia can occur during late gestation, post-natal period, or with mature brain when an astrocytic proliferation response is possible.
Dyke-Davidoff-Masson syndrome
Atrophy/encephalomalacia of one cerebral hemisphere with compensatory dilation of the ipsilateral lateral ventricle; unilateral ipsilateral decrease in size of cranial fossa associated with thickened calvarium, with or without enlargement of ipsilateral paranasal sinuses.
Prenatal, congenital, or acquired ischemic disorder resulting in unilateral atrophy of one cerebral hemisphere; rare disorder in adolescents presenting with seizures, mental retardation, and hemiparesis.
Brain atrophy often most pronounced in frontal and temporal lobes; sulcal and ventricular prominence. Cortical atrophic changes common.
Acquired dementia much less common than Alzheimer disease. Histopathologic findings or neuronal loss and cytoplasmic inclusion bodies (Pick bodies).
Huntington disease
Disproportionate atrophy of basal ganglia (caudate > putamen > cerebellum/brainstem); variable decreased attenuation involving the putamen bilaterally; usually no contrast enhancement.
Autosomal dominant neurodegenerative disease usually presenting after age 40 y with progressive movement disorders and behavioral and mental dysfunction.
Disproportionately greater prominence of the ventricles relative to the sulci.
Dilation of the ventricles with transependymal egress of CSF thought to be secondary to impaired resorption of CSF through arachnoid granulations. Associated with progressive memory impairment, urinary incontinence, and gait disorders.
Enlargement of ventricles above site of obstruction to CSF flow.
Blockage of ventricular shunt catheters can result in progressive ventricular dilation.
Fig. 2.7a, b Chiari II malformation. Axial (a) and sagittal (b) images show enlarged ventricles from hydrocephalus-related herniation of the cerebellum through the foramen magnum related to the Chiari II malformation.Fig. 2.8 Dandy-Walker malformation. Axial image shows the absence of the cerebellar vermis, enlarged unroofed fourth ventricle, and hypoplasia of the cerebellar hemispheres.Fig. 2.9 Colpocephaly. Axial image in a young child with dysgenesis of the corpus callosum and enlarged occipital horns of the lateral ventricles.Fig. 2.10 Medulloblastoma. Axial image shows the tumor extending from the vermis into the fourth ventricle, resulting in hydrocephalus.Fig. 2.11a, b Choroid plexus carcinoma. Axial postcontrast images show a large enhancing tumor in the right lateral ventricle associated with ventricular dilation.Fig. 2.12 Choroid plexus papilloma. Axial image in a 3-year-old boy shows the tumor in the right lateral ventricle associated with ventricular dilation from overproduction of cerebrospinal fluid (CSF) by the tumor.Fig. 2.13a, b Intraventricular arachnoid cyst. Axial images show the arachnoid cyst in the third and left lateral ventricles associated with hydrocephalus.Fig. 2.14a–d Ventriculitis. Axial postcontrast CT image (a) shows abnormal enhancement along the frontal horn of the left lateral ventricle. Abnormal high signal on axial fluid attenuation inversion recovery (FLAIR) MRI (b), restricted diffusion on axial diffusion-weighted MRI (c), and abnormal contrast enhancement on axial T1-weighted MRI (d) are seen along the ependymal margin of the left lateral ventricle.Fig. 2.15 Intraventricular hemorrhage. Axial image shows high attenuation from acute hemorrhage within dilated lateral ventricles.Fig. 2.16 Porencephaly. Axial image shows dilated lateral ventricles and a porencephalic cyst on the right.Fig. 2.17 Encephalomalacia. Dilation of the left lateral ventricle secondary to encephalomalacia from old infarction in the vascular distribution of the left middle cerebral artery.Fig. 2.18 Encephalomalacia, cerebritis. Dilation of the lateral ventricles in a neonate secondary to encephalomalacia from destructive changes of cerebritis.Fig. 2.19 Alzheimer disease. Axial image shows asymmetric cerebral atrophy involving the frontal and temporal lobes with compensatory dilation of the ventricles.Fig. 2.20 Pick disease. Axial image shows asymmetric cerebral atrophy involving the frontal lobes with compensatory dilation of the ventricles.Fig. 2.21a, b Normal pressure hydrocephalus. Axial images show asymmetric prominence of the ventricles relative to the sulci.Fig. 2.22 Ventricular shunt failure. Axial image shows an intraventricular shunt with abnormally dilated ventricles.
Table 2.6 Abnormal or altered configurations of the ventricles
Lesions
CT Findings
Comments
Congenital, developmental, or acquired
Cephaloceles (meningoceles or meningoencephaloceles)
Defect in skull through which there is either herniation of meninges and CSF (meningocele) or meninges, CSF, and brain tissue (meningoencephaloceles).
Congenital malformation involving lack of separation of neuroectoderm from surface ectoderm with resultant localized failure of bone formation. Occipital location most common in Western hemisphere, frontoethmoidal location most common site in Southeast Asians. Other sites include parietal and sphenoid bones. Cephaloceles can also result from trauma or surgery.
Alobar: Large monoventricle with posterior midline cyst; lack of hemisphere formation with absence of falx, corpus callosum, and septum pellucidum. Fused thalami.
Semilobar: Monoventricle with partial formation of interhemispheric fissure, occipital and temporal horns, partially fused thalami. Absent corpus callosum and septum pellucidum. Associated with mild craniofacial anomalies.
Lobar: Near complete formation of interhemispheric fissure and ventricles. Fused inferior portions of frontal lobes, dysgenesis of corpus callosum, absence of septum pellucidum, separate thalami, neuronal migration disorders.
Septo-optic dysplasia (de Morsier syndrome):
Mild form of lobar holoprosencephaly. Dysgenesis or agenesis of septum pellucidum, optic nerve hypoplasia, squared frontal horns; association with schizencephaly in 50%.
Holoprosencephaly: Disorders of diverticulation (weeks 4–6 of gestation) characterized by absent or partial cleavage and differentiation of the embryonic cerebrum (prosencephalon) into hemispheres and lobes.
Absent or incomplete formation of gyri and sulci with shallow sylvian fissures and “figure 8” appearance of brain on axial images, abnormally thick cortex, gray matter heterotopia with smooth gray-white matter interface.
Severe disorder of neuronal migration (occurs during weeks 7–16 of gestation) with absent or incomplete formation of gyri, sulci, and sylvian fissures. Typically in association with microcephaly (defined as head circumference 3 standard deviations below normal). Associated with severe mental retardation, developmental delay, seizures, and early death.
Nodular heterotopia appears as one or more nodules of isodense gray matter along the ventricles or within the cerebral white matter.
Disorder of neuronal migration (weeks 7–22 of gestation) in which a collection or layer of neurons is located between the ventricles and cerebral cortex. Can have a bandlike (laminar) or nodular appearance isointense to gray matter; may be unilateral or bilateral. Associated with seizures, schizencephaly.
Cleft in the brain extending from the ventricle to cortical surface lined by heterotopic gray matter; may be narrow (closed lip) or wide (open lip).
Association with seizures, blindness, retardation, and other CNS anomalies (septo-optic dysplasia, etc.). Clinical manifestations related to severity of malformation. Ischemia or insult to portion or germinal matrix before hemisphere formation.
Nodular or multinodular region of gray matter heterotopia involving all or part of a cerebral hemisphere with associated enlargement of the ipsilateral lateral ventricle and hemisphere.
Neuronal migration disorder associated with hamartomatous overgrowth of the involved hemisphere.
Chiari II malformation (Arnold-Chiari malformation)
Small posterior cranial fossa with gaping foramen magnum through which there is an inferiorly positioned vermis associated with a cervicomedullary kink. Beaked dorsal margin of the tectal plate. Myelomeningoceles in nearly all patients. Hydrocephalus and syringomyelia are common. Dilated lateral ventricles posteriorly (colpocephaly).
Complex anomaly involving the cerebrum, cerebellum, brainstem, spinal cord, ventricles, skull, and dura. Failure of fetal neural tube to develop properly results in altered development affecting multiple sites of the CNS.
Vermian aplasia or severe hypoplasia; communication of fourth ventricle with retrocerebellar cyst; enlarged posterior fossa, high position of tentorium and transverse venous sinuses. Hydrocephalus common. Associated with other anomalies such as dysgenesis of the corpus callosum, gray matter heterotopia, schizencephaly, holoprosencephaly, and cephaloceles.
Abnormal formation of the roof of the fourth ventricle with absent or near incomplete formation of cerebellar vermis.
Spectrum of abnormalities ranging from complete to partial absence of the corpus callosum. Widely separated and parallel orientations of frontal horns and bodies of lateral ventricles; high position of third ventricle in relation to interhemispheric fissure, colpocephaly. Associated with interhemispheric cysts, lipomas, and anomalies such as Chiari II malformation, gray matter heterotopia, Dandy-Walker malformations, holoprosencephaly, azygous anterior cerebral artery, and cephaloceles.
Failure or incomplete formation of corpus callosum (weeks 7–18 of gestation). Axons that normally cross from one hemisphere to the other are aligned parallel along the medial walls of the lateral ventricles (bundles of Probst).
Irregular, relatively well-circumscribed zone with low attenuation similar to CSF, surrounded by poorly defined thin zone of decreased attenuation in adjacent brain tissue; no contrast enhancement or peripheral edema.
Represents remote sites of brain injury (trauma, infarction, infection, or hemorrhage) with evolution into a cystic zone with CSF surrounded by gliosis in adjacent brain parenchyma.
Neuroepithelial cyst
Well-circumscribed cysts with low attenuation, thin walls; no contrast enhancement or peripheral edema.
Cyst walls have histopathologic features similar to epithelium; neuroepithelial cysts located in choroid plexus > choroidal fissure > ventricles > brain parenchyma.
Subependymal hamartomas: Small nodules located along and projecting into the lateral ventricles with or without calcifications; MRI signal on T1- and T2-weighted images similar to cortical tubers; gadolinium enhancement common.
Cortical and subependymal hamartomas are nonmalignant lesions associated with tuberous sclerosis.
Compression and shift of the lateral and third ventricles under the falx cerebri to the other side, with or without dilation of contralateral lateral ventricle because of CSF outflow obstruction from compression at the contralateral foramen of Monro; with or without displacement of ipsilateral anterior cerebral artery and subependymal veins.
Most often occurs from primary or metastatic intra-axial tumor or hemorrhage.
Ascending type: Upward herniation of cerebellar vermis and hemispheres through the tentorial incisura, resulting in compression and displacement of the cerebral aqueduct and posterior portion of the third ventricle, effacement of superior vermian cistern, compression and anterior displacement of the fourth ventricle; with or without obstructive hydrocephalus.
Descending type: Medial and inferior displacement of uncus and parahippocampal gyrus below the tentorium; progressive effacement of suprasellar cistern and basal cisterns, compression of ipsilateral portion of the midbrain that is displaced toward contralateral side; with or without Kernohan notch; with or without Duret hemorrhage; with or without inferior displacement and/or compression of anterior choroidal, posterior communicating, and posterior cerebral arteries, as well as perforating branches of the basilar artery, resulting in cerebral, cerebellar, and/or brainstem infarcts. Often results in death.
Descending type more common than ascending type. Typically results from a focal mass lesion or hemorrhage, causing displacement of brain tissue across tentorium.
Cavum septum pellucidum: CSF-containing zone between two septal leaves.
Cavum vergae: Same as cavum septum pellucidum with posterior extension of fluid-containing zone between septal leaves.
Developmental anomalies with lack of normal involution of fetal cavities separating the two septal leaves; occurs in 3% of normal adults; no clinical significance.
Fig. 2.23 Meningoencephalocele. Axial image shows a parietal meningoencephalocele.Fig. 2.24a, b Lobar holoprosencephaly. Axial images show fusion of the anteroinferior portions of the frontal lobes (a) with separation of the upper portions of the frontal lobes (b) with an interhemispheric fissure.Fig. 2.25 Lissencephaly. Axial image shows the absence of gyri and sulci and the lack of normal gray-white matter demarcation.Fig. 2.26 Nodular gray matter heterotopia. Axial image shows nodular zones with intermediate attenuation along the margins of the lateral ventricles representing gray matter heterotopia.Fig. 2.27a, b Schizencephaly. Axial image (a) shows open lip schizencephaly lined by gray matter along the margins. Axial image (b) in a young child with congenital toxoplasmosis with closed lip schizencephaly on the left, dystrophic calcifications at sites of prior infection, and encephaloclastic changes (arrow).Fig. 2.28 Unilateral hemimegalencephaly. Axial image shows enlargement of the left cerebral hemisphere with abnormal gyral configuration and zones of decreased attenuation in the left frontal lobe.Fig. 2.29a–c Chiari II malformation. Sagittal (a), coronal (b), and axial (c) images show an intraventricular shunt and changes associated with a Chiari II malformation, as well as an abnormally shaped fourth ventricle. Axial image in another patient shows colpocephaly.Fig. 2.30a, b Dandy-Walker malformation. Axial CT image (a) and coronal T1-weighted MRI (b) show the absence of the vermis and hypoplasia of the cerebellar hemispheres with altered shape of the fourth ventricle.Fig. 2.31a, b Dysgenesis of the corpus callosum. Axial images show widely separated lateral ventricles related to bundles of Probst.Fig. 2.32 Porencephalic cyst. Axial image shows abnormal enlargement of the right lateral ventricle from prior infection and localized brain destruction with dystrophic calcifications and a porencephalic cyst.Fig. 2.33 Hamartomas, tuberous sclerosis. Axial image shows multiple calcified ependymal hamartomas.
Well-circumscribed extra-axial lesions with low attenuation signal similar to CSF; no central enhancement, thin linear peripheral contrast enhancement; rarely atypical appearance with proteinaceous contents: intermediate, slightly high attenuation.
Common usually incidental nonneoplastic cyst in pineal gland.
Well-circumscribed spheroid lesions located at the anterior portion of the third ventricle; variable attenuation (low, intermediate, or high); usually no contrast enhancement.
Benign epithelial-lined cysts; common presentation of headaches and intermittent hydrocephalus; removal leads to cure.
Neuroepithelial cyst
Well-circumscribed cysts with low attenuation, thin walls; no contrast enhancement or peripheral edema.
Cyst walls have histopathologic features similar to epithelium; neuroepithelial cysts located in choroid plexus > choroidal fissure > ventricles > brain parenchyma.
Well-circumscribed cysts with low attenuation equal to CSF; thin walls; no contrast enhancement or peripheral edema.
Cyst walls have histopathologic features of arachnoid; can arise from choroid plexus or extension of arachnoid from choroidal fissure into ventricles.
Intraventricular epidermoid
Well-circumscribed spheroid or multilobulated, extra-axial ectodermal inclusion cystic lesions with low to intermediate attenuation, no contrast enhancement, with or without bone erosion/destruction. Often insinuate along CSF pathways; chronic deformation of adjacent neural tissue.
Nonneoplastic congenital or acquired extra-axial off-midline lesions filled with desquamated cells and keratinaceous debris; usually mild mass effect on adjacent brain; infratentorial > supratentorial locations. Adults: men = women; with or without related clinical symptoms.
Nodular heterotopia appears as one or more nodules of gray matter attenuation along the ventricles or within the cerebral white matter.
Disorder of neuronal migration (weeks 7–22 of gestation) in which a collection or layer of neurons is located between the ventricles and cerebral cortex. Can have a bandlike (laminar) or nodular appearance with attenuation similar to gray matter; may be unilateral or bilateral. Associated with seizures, schizencephaly.
Single or multiple well-circumscribed or poorly defined lesions involving the brain, skull, dura, leptomeninges, choroid plexus/ventricles, or pituitary gland; low to intermediate attenuation usually with contrast enhancement, with or without bone destruction, with or without compression of neural tissue or vessels. Leptomeningeal tumor often best seen on postcontrast images.
Metastatic tumor may have variable destructive or infiltrative changes involving single or multiple sites of involvement. Disseminated tumor within the ventricles can result from primary CNS tumors or extraneural primary neoplasms.
Extra-axial dural-based lesions, well-circumscribed; supratentorial > infratentorial, parasagittal > convexity > sphenoid ridge > parasellar > posterior fossa > optic nerve sheath > intraventricular; intermediate attenuation, usually prominent contrast enhancement, with or without calcifications.
Most common extra-axial tumor; usually benign neoplasms; typically occurs in adults (> 40 y), women > men. Multiple meningiomas seen with neurofibromatosis type 2; can result in compression of adjacent brain parenchyma, encasement of arteries, and compression of dural venous sinuses; rarely invasive/malignant types.
Extra-axial mass lesions, often well circumscribed; intermediate attenuation, prominent contrast enhancement (may resemble meningiomas), with or without associated erosive bone changes.
Rare neoplasms in young adults (males > females) sometimes referred to as angioblastic meningioma or meningeal hemangiopericytoma; arise from vascular cells/pericytes; frequency of metastases > meningiomas.
Central neurocytoma
Circumscribed lesion located at the margin of the lateral ventricle or septum pellucidum with intraventricular protrusion, heterogeneous intermediate attenuation; with or without calcifications and/or small cysts; heterogeneous contrast enhancement.
Rare tumors that have neuronal differentiation; imaging appearance similar to intraventricular oligodendrogliomas; occur in young adults; benign slow-growing lesions.
Astrocytoma
Low-grade astrocytoma: Focal or diffuse mass lesion usually located in cerebral or cerebellar white matter or brainstem with low to intermediate attenuation, with or without mild contrast enhancement. Minimal associated mass effect. May extend into ventricles.
Juvenile pilocytic astrocytoma subtype: Solid/cystic focal lesion with low to intermediate attenuation, usually with prominent contrast enhancement. Lesions located in the cerebellum and brainstem. May extend into ventricles.
Often occur in children and adults (age 20–40 y). Tumors comprised of well-differentiated astrocytes. Association with neurofibromatosis type 1; 10-y survival common; may become malignant.
Common in children; usually favorable prognosis if totally resected.
Gliomatosis cerebri: Infiltrative lesion with poorly defined margins with mass effect located in the white matter, with low to intermediate attenuation; usually no contrast enhancement until late in disease. May extend into ventricles.
Anaplastic astrocytoma: Often irregularly marginated lesion located in the white matter with low to intermediate attenuation, with or without contrast enhancement. May extend into ventricles.
Diffusely infiltrating astrocytoma with relative preservation of underlying brain architecture. Imaging appearance may be more prognostic than histologic grade; ~2-y survival. Intermediate between low-grade astrocytoma and glioblastoma multiforme; ~2-y survival.
Glioblastoma multiforme: Irregularly marginated mass lesion with necrosis or cyst; mixed low and intermediate attenuation, with or without hemorrhage; prominent heterogeneous contrast enhancement, peripheral edema; can cross corpus callosum.
Most common primary CNS tumor; highly malignant neoplasms with necrosis and vascular proliferation, usually seen in patients older than 50 y; extent of lesion underestimated by CT; survival < 1 y.
Circumscribed lesion located near the foramen of Monro with mixed low to intermediate attenuation, with or without cysts and/or calcifications, with heterogeneous contrast enhancement.
Subependymal hamartoma near the foramen of Monro; occurs in 15% of patients with tuberous sclerosis younger than 20 y; slow-growing lesions that can progressively cause obstruction of CSF flow through the foramen of Monro; long-term survival usual if resected.
Circumscribed, lobulated lesions; both suprasellar and intrasellar location > suprasellar > intrasellar; can extend into the third ventricle; variable low, intermediate, and/or high attenuation; with or without nodular or rim contrast enhancement. May contain cysts, lipid components, and calcifications.
Usually histologically benign but locally aggressive lesions arising from squamous epithelial rests along the Rathke cleft; occurs in children (5–15 y) and adults (> 40 y), males = females.
Medulloblastoma (primitive neuroectodermal tumor of the cerebellum)
Circumscribed spheroid or lobulated infratentorial lesion, usually in the fourth ventricle, with or without cysts and/or calcifications; low or intermediate attenuation, variable contrast enhancement, with or without extension through the foramina of Luschka and Magendie.
Occurs more commonly in children than adults; two thirds infratentorial, one third supratentorial.
Circumscribed intraventricular lesions with intermediate attenuation, typically no contrast enhancement; can occasionally cause obstructive hydrocephalus.
Rare benign (World Health Organization [WHO] grade 1) lesions consisting of astrocytes and ependymal cells arising from below the ventricular lining with protrusion into the ventricles (fourth > lateral > third ventricles); can involve the septum pellucidum. Usually occurs in adults, male/female ratio of 2.3:1.
Oligodendroglioma
Circumscribed lesion with mixed low to intermediate attenuation; may have areas of clumplike calcification; heterogeneous contrast enhancement; involves white matter and cerebral cortex; can cause chronic erosion of inner table of calvarium; also occurs within ventricles.
Uncommon slow-growing gliomas with usually mixed histologic patterns (astrocytoma, etc.). Usually seen in adults older than 35 y; 85% supratentorial. If low-grade, 75% 5-y survival; higher grade lesions have a worse prognosis.
Tumors often have intermediate attenuation to intermediate to slightly high attenuation, with contrast enhancement, with or without central and/or peripheral calcifications. Malignant tumors are often larger than benign pineal lesions (pineocytoma), as well as heterogeneous attenuation and contrast enhancement pattern; with or without leptomeningeal tumor.
Pineal gland tumors account for 8% of intracranial tumors in children and 1% of tumors in adults; 40% of tumors are germinomas, followed by pineoblastoma and pineocytoma, teratoma, choriocarcinoma, endodermal sinus tumor, astrocytoma, and metastatic tumor.
Circumscribed tumors with or without disseminated disease; pineal region > suprasellar region > third ventricle/basal ganglia; low to intermediate attenuation, with or without cystic like regions; usually with contrast enhancement of tumor and leptomeninges (if disseminated).
Most common type of germ cell tumor; occurs in males > females (age 10–30 y); usually midline neoplasms.
Circumscribed and/or lobulated lesions with papillary projections; intermediate attenuation; usually prominent contrast enhancement, with or without calcifications. Locations: atrium of lateral ventricle (children) > fourth ventricle (adults), rarely other locations such as the third ventricle; associated with hydrocephalus.
Rare intracranial neoplasms; CT features of choroid plexus carcinoma and papilloma overlap; both histologic types can disseminate along CSF pathways and invade brain tissue.
Circumscribed mass lesions with intermediate attenuation, with or without zones of high attenuation from hemorrhage and/or calcifications; usually show contrast enhancement.
Rare malignant tumors involving the CNS usually occurring in the first decade. Histologically appear as solid tumors with or without necrotic areas, similar to malignant rhabdoid tumors of the kidney. Associated with a poor prognosis.
Single or multiple solid and/or cystic lesions located in basal ganglia and/or corticomedullary junctions in cerebral hemispheres, rarely in ventricles; low to intermediate attenuation; nodular or rim pattern of contrast enhancement; with or without peripheral edema.
Most common opportunistic CNS infection in AIDS patients; caused by ingestion of food contaminated with parasites (Toxoplasma gondii).
Cysticercosis
Single or multiple cystic lesions in brain, meninges, occasionally in ventricles.
Acute/subacute phase: Low to intermediate attenuation; with or without nodular pattern of contrast enhancement; with or without peripheral edema.
Chronic phase: Calcified granulomas.
Caused by ingestion of ova (Taenia solium) in contaminated food (undercooked pork); involves meninges > brain parenchyma > ventricles.
Hydatid cyst
Echinococcus granulosus: Single or rarely multiple cystic lesions with a thin wall with low attenuation; typically no contrast enhancement or peripheral edema unless super-infected; often located in vascular territory of the middle cerebral artery.
Echinococcus multilocularis: Cystic (with or without multilocular) and/or solid lesions; central zone of intermediate attenuation surrounded by a slightly thickened rim, with contrast enhancement; peripheral zone of edema and calcifications are common.
Caused by parasites E. granulosus (South America, Middle East, Australia, and New Zealand) or E. multilocularis (North America, Europe, Turkey, and China). CNS involvement in 2% of cases of hydatid infestation.
Poorly marginated extra-axial lesion with low to intermediate attenuation; usually shows contrast enhancement, with localized mass effect and peripheral edema. Often associated with contrast enhancement in the leptomeninges with or without ventricles.
Multisystem noncaseating granulomatous disease of uncertain cause that can involve the CNS in 5% to 15% of cases. Associated with severe neurologic deficits if untreated.
Lesions with irregular margins that can be located in the brain parenchyma, dura, and/or ventricles.
CT: AVMs contain multiple tortuous tubular vessels that have intermediate or slightly increased attenuation that show contrast enhancement. Calcifications occur in 30%. Computed tomography angiography (CTA) shows arteries, veins, and nidus of AVM even when there is hemorrhage.
Supratentorial AVMs occur more frequently (80%–90%) than infratentorial AVMs (10%–20%). Annual risk of hemorrhage. AVMs can be sporadic, congenital, or associated with a history of trauma. Multiple AVMs can be seen in syndromes: Rendu-Osler-Weber (AVMs in brain and lungs and mucosal, capillary telangiectasias) and Wyburn-Mason (AVMs in brain and retina, with cutaneous nevi).
Multiple tortuous blood vessels involving choroidal and thalamoperforate arteries, internal cerebral veins, vein of Galen (aneurysmal formation), straight and transverse venous sinuses, and other adjacent veins and arteries. The venous portions often show contrast enhancement. CTA can show patent portions of the vascular malformation.
Heterogeneous group of vascular malformations with arteriovenous shunts and dilated deep venous structures draining into and from an enlarged vein of Galen, with or without hydrocephalus, with or without hemorrhage, with or without macrocephaly, with or without parenchymal vascular malformation components, with or without seizures; high-output congestive heart failure in neonates.
Prominent localized unilateral leptomeningeal enhancement usually in parietal and/or occipital regions in children; with or without gyral enhancement; mild localized atrophic changes in brain adjacent to the pial angioma; with or without prominent medullary and/or subependymal veins; with or without ipsilateral prominence of choroid plexus. Gyral calcifications > 2 y; progressive cerebral atrophy in region of pial angioma.
Also known as encephalotrigeminal angiomatosis, neurocutaneous syndrome associated with ipsilateral “port wine” cutaneous lesion and seizures; results from persistence of primitive leptomeningeal venous drainage (pial angioma) and developmental lack of normal cortical veins, producing chronic venous congestion and ischemia.
Fig. 2.34 Subfalcine herniation. Axial image shows a left-sided subdural hematoma with subfalcine herniation rightward.Fig. 2.35 Transtentorial herniation. Axial image shows a large hematoma in the left temporal lobe extending into the left lateral ventricle associated with mass effect causing counterclockwise rotation of the midbrain and transtentorial/uncal herniation.Fig. 2.36 Cavum vergae. Axial image shows separation of the two leaves of the septum pellucidum extending posteriorly (arrows).Fig. 2.37 Pineal cyst. Axial image shows a pineal cyst causing hydrocephalus.Fig. 2.38a, b Colloid cyst. Axial pre- (a) and postcontrast (b) images show a colloid cyst with high attenuation in the anterior upper portion of the third ventricle.Fig. 2.39a–d Intraventricular arachnoid cyst. Axial CT (a–c) and axial T2-weighted MRI (d) images show an arachnoid cyst in the third and left lateral ventricles causing hydro-cephalus.Fig. 2.40 Gray matter heterotopia. Axial image shows multiple nodular zones of gray matter heterotopia along the lateral ventricles.Fig. 2.41 Tuberous sclerosis, ependymal hamartomas. Axial image shows multiple calcified ependymal hamartomas.Fig. 2.42a, b Metastatic tumor. Axial postcontrast images show enhancing subarachnoid and intraventricular tumor from pineoblastoma.Fig. 2.43 Meningioma. Axial post-contrast image shows an enhancing tumor involving the posterior portion of the third ventricle.Fig. 2.44 Hemangiopericytoma. Axial postcontrast image shows an enhancing lesion involving the posterior portion of the left lateral ventricle.Fig. 2.45 Malignant astrocytoma. Axial postcontrast image shows an enhancing lesion in the right occipital lobe extending into the splenium of the corpus callosum.Fig. 2.46 Giant cell astrocytoma, tuberous sclerosis. Axial image shows a tumor at the right foramen of Monro (arrow), as well as multiple calcified ependymal hamartomas.Fig. 2.47 Craniopharyngioma. Sagittal postcontrast image shows a complex lesion in the suprasellar cistern involving the third ventricle.Fig. 2.48 Medulloblastoma. Axial image shows the tumor in the vermis extending into the fourth ventricle, causing hydrocephalus.Fig. 2.49a, b Ependymoma. Axial images in two different patients show ependymomas in the fourth ventricle (a) and left lateral ventricle (b).Fig. 2.50 Subependymoma. Axial image shows a tumor in the frontal horn of the right lateral ventricle.Fig. 2.51a, b Pineal gland tumors. Axial images show a pineoblastoma (a) and pineal teratoma (b) associated with dilated ventricles.Fig. 2.52 Germ cell tumors. Axial image shows a germinoma in the third ventricle.Fig. 2.53a, b Choroid plexus papilloma. Axial pre- (a) and postcontrast (b) images show an enhancing tumor in the third ventricle.Fig. 2.54 Choroid plexus carcinoma. Axial postcontrast image shows a large enhancing tumor in the right lateral ventricle.Fig. 2.55 Atypical teratoid/rhabdoid tumor. Axial postcontrast image shows a complex enhancing solid and cystic lesion in the fourth ventricle.Fig. 2.56a, b Toxoplasmosis. Axial images show multiple calcifications from healed granulomas in two different patients.Fig. 2.57a–c Sarcoid. Axial postcontrast CT image (a) shows enhancement along the atrium and occipital horn of the left lateral ventricle. Corresponding abnormal increased signal and contrast enhancement are seen on an axial FLAIR MRI (b) and an axial T1-weighted image (c), respectively.Fig. 2.58a, b Arteriovenous malformation (AVM). Axial image (a) shows a calcified AVM in the left cerebral hemisphere with hemorrhage into the ventricles. Axial computed tomography angiography (CTA) image (b) shows the abnormal collection of vessels of the AVM.Fig. 2.59 Vein of Galen aneurysm. Axial postcontrast image shows an abnormally enlarged enhancing vein of Galen and straight venous sinus.Fig. 2.60 Sturge-Weber syndrome. Axial postcontrast image shows enlarged enhancing medullary and ependymal veins.
Only gold members can continue reading. Log In or Register to continue