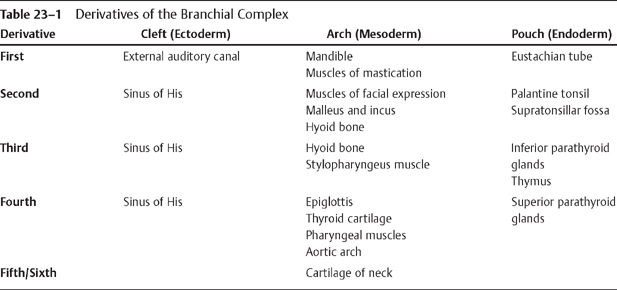
CASE 23 A 4-year-old male presents with a nontender right-sided neck mass. Figure 23A Contrast-enhanced axial CT images (Figs. 23A1 and 23A2) depict a well-demarcated, hypodense right-sided unilocular mass effacing the anterior margin of the right sternocleidomastoid muscle. The mass displaces the right internal carotid artery and jugular vein medially. The mass extends inferiorly from the level of the mandibular angle and displaces the right submandibular gland anteriorly. There is a thin enhancing rim, whereas centrally the lesion is nearly isointense with CSF. There is minimal associated lymphadenopathy. Second branchial cleft cyst (BCC) Pertains to cystic neck masses as follows: Embryologically, the branchial complex consists of six, paired mesodermal arches, which are separated by five clefts lined by endoderm. The fifth and sixth arches are generally rudimentary; however, the first four develop the major structures of the neck, as outlined in Table 23-1. There are three general types of anomalies of the branchial cleft complex. Branchial cleft sinuses are tracts, with or without a cyst, that communicate to gut or skin. Fistulae are residual tracts extending from pharynx to the skin. BCCs are isolated and have no opening to skin or pharynx. A second BCC can arise anywhere along the embryologic path of the second branchial cleft fistula, which runs from the tonsillar fossa inferiorly along the anterior border of the sternocleidomastoid muscle to the supraclavicular location. There are four types of second BCCs based on their location along this embryologic pathway. Fistulae of second BCCs generally end around the supratonsillar fossa/pillar or directly on tonsil surface and present with recurrent attacks of inflammation.
Clinical Presentation
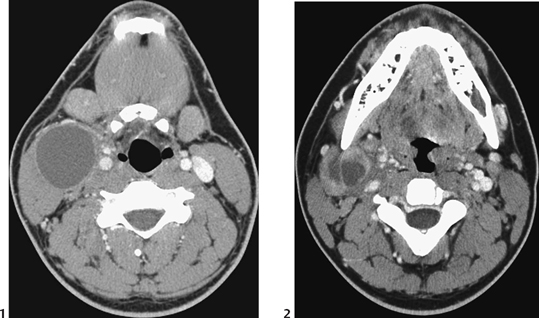
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Etiology
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


