23 Incidental Meningioma
23.1 Introduction
As the quality and accessibility of diagnostic imaging has increased, so has the number of incidental findings that require management. Incidental findings are unrelated to the original purpose of the examination. Meningiomas are one of the most common brain tumors to be detected incidentally because they can be small in size and asymptomatic. Management of these tumors may include observation, radiation, or surgery. Many of these tumors can be managed conservatively. However, a small proportion of meningiomas with high growth rate or concerning location and patient demographics are best treated with early surgical resection.
In this chapter, we present the radiographic findings and management of two cases of meningioma that presented incidentally. We start with the radiographic analysis and include conventional imaging pearls that help distinguish between the different entities within the differential diagnosis. We include a companion case of meningioma that was followed up with imaging to explore the factors affecting growth potential and ultimate follow-up time frame for incidentally found meningiomas.
23.2 Case Presentation
23.2.1 History and Physical Examination
A 37-year-old with history of motor vehicle accident has head CT for scalp laceration. MRI was done afterward for incidental finding on head CT.
The neurological examination was normal.
23.2.2 Imaging Findings
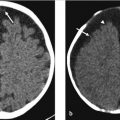
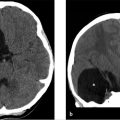
Contrast MRI brain shows a large extra-axial mass of an approximate size of 4.5 × 5.2 cm in the right parieto-occipital region. The mass is isointense on T2-weighted imaging (T2WI; ▶ Fig. 23.1a), hypointense on T1WI (▶ Fig. 23.1b), and hyperintense on fluid-attenuated inversion recovery (FLAIR; ▶ Fig. 23.1c), and enhances homogeneously with a dural tail (white arrow in ▶ Fig. 23.1e, f).

Diagnosis: Right parieto-occipital meningioma.
23.2.3 Additional Tests to Consider
N o additional tests are recommended.
23.3 Neurosurgical Consultation
There is a large right parieto-occipital convexity meningioma in a relatively young and healthy woman, so surgical intervention was offered. The lesion is in a very surgically accessible region and does not yet involve any key vascular or neuronal structures. The risk of growth is moderately high with this tumor. Surgical resection at this time would allow for operating on the tumor while the risk is relatively low as well as provide a tissue diagnosis to guide further treatment. Stereotactic radiosurgery would not be offered for this lesion because it is larger than 3 cm and there is an increased risk of posttreatment edema and radiation necrosis.
23.4 Differential Diagnosis of Dural Based Masses
Meningioma:
On CT often hyperdense, may calcify, and often associated with hyperostosis and dilatation of the adjacent paranasal sinuses.
On MRI, homogeneous enhancement, usually isointense T1/T2, and dural tail may be seen but not pathognomonic.
Metastatic disease to dura:
Frequently multiple with infiltrating behavior and extensive adjacent dural thickening rather than a well-defined globular mass.
Sarcoid:
Associated leptomeningeal enhancement, thickened pituitary stalk, clinical features present including elevated angiotensin-converting enzyme (ACE) and abnormal chest X-ray.
Hemangiopericytoma/solitary fibrous tumor:
Often invades bone and appears more aggressive.
Demonstrates microlobulation and extensive peripheral vascularity.
Primary dural lymphoma:
Often multifocal without calvarial invasion.
Demonstrates restricted diffusion and T2 low signal due to hypercellularity.
23.5 Diagnostic Pearls and Pitfalls
Meningioma is one of few tumors that have distinct female predominance.
Association with prior radiation.
The dural tail is NOT pathognomonic and may be seen in PXA, lymphoma, and pituitary adenoma, as well as granulomatous/inflammatory conditions such as sarcoidosis.
No reliable way to distinguish between malignant and typical meningiomas; however, factors associated with increased growth potential include increased signal on T2WI, extensive surrounding edema, younger-age patient, absence of calcification, and recurrent lesions. Features suggesting less growth potential include smaller size, highly calcified lesion, and older-age patient.
Close inspection of dural venous sinus when meningioma is in close proximity is important as meningiomas may occlude the sinus. Determination as to the patency of the sinus is important for surgical planning.
Consider neurofibromatosis type 2 (NF2) if the patient presents with meningioma and any of the following: cataract, schwannoma, glioma, and a parent, sibling, or child with NF2; or if the patient had vestibular schwannoma diagnosed at younger 30 years of age; or if the patient had multiple meningiomas and any of the following: vestibular schwannoma diagnosed before the age of 30 years, cataract, or glioma.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


