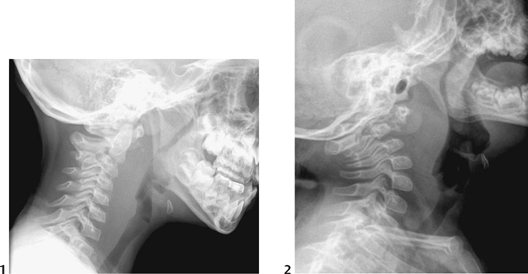
CASE 26 A 23-month-old boy presents with head tilt, fever, and right-sided cervical lymphadenopathy. Figure 26A Figure 26B Lateral soft tissue radiograph of the neck shows increased thickness of the prevertebral soft tissues anterior to the upper cervical spine, worrisome for retropharyngeal inflammation, either abscess or cellulitis (Fig. 26A). CT study was performed under general anesthesia with an orotracheal tube in situ. Enhanced axial CT image shows a large, well-delineated right-sided mass with low-intensity interior and thick enhancing rim (Fig. 26B). There is bowing of the right internal carotid artery anterolaterally and compression of the right internal jugular vein. Mass effect is present on the right posterolateral aspect of the oropharynx, with moderate deviation of the right tonsil anteromedially. Remaining CT images show that the lesion extends from the skull base inferiorly down to the level of the mandible and into the right parapharyngeal space. Large right-sided retropharyngeal abscess (RPA) The retropharyngeal area is a deep neck space extending from the skull base down into the mediastinum that normally contains lymph nodes in young children. It is bordered by buccopharyngeal fascia anteriorly, prevertebral fascia posteriorly, and carotid sheaths laterally. RPAs are potentially life-threatening deep space neck infections, which can be of medical or traumatic origin. Infrequent in occurrence, retropharyngeal infection and abscess is largely a disease of childhood, with most cases occurring in children <5 years of life. Most RPAs result from lymphatic spread of a variety of predisposing head and neck and upper respiratory tract infections, including pharyngitis and tonsillitis. Traumatic causes may follow lacerations from objects stuck in the mouth such as pencils. In early childhood, lymph nodes are located in the retropharyngeal space, generally straddling the junction of retropharyngeal and parapharyngeal spaces. Lymphadenitis in this region can subsequently lead to cellulitis, phlegmon, and abscess. With increasing age, atrophy of the retropharyngeal lymph nodes probably occurs, decreasing the disease risk in older children. Infection in older children and adults is more often due to perforation from foreign bodies and iatrogenic injury including endoscopy. The typical presentation of retropharyngeal infection and abscess is often nonspecific, with sore throat, fever, torticollis, and neck pain commonly seen. Drooling, malaise, decreased oral intake, irritability, neck mass, and respiratory distress or stridor, decreased appetite, jaw stiffness or neck stiffness, or muffled voice can also be seen. Occasionally, upper respiratory infection can precede symptoms of RPA. Physical findings include fever, cervical adenopathy, decreased range of neck motion, neck mass, posterior pharyngeal mass, and respiratory distress. Positive microbiological cultures of pus, blood, or pharyngeal space are found in roughly 50% of patients. Predominant organisms include Streptococcus species and Staphylococcus aureus. However, anaerobes and mixed flora can also be seen. Figure 26C Two patients with RPAs and differing appearance of retropharyngeal soft tissues. The patient on the left (1) shows moderate diffuse soft tissue thickening and displacement of the air column anteriorly. The patient on the right (2) shows more marked soft tissue bulging superiorly and abnormality at the craniocervical junction.
Clinical Presentation


Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Clinical Findings
Pathology and Laboratory Findings
Imaging Findings
RADIOGRAPHY
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


