Diagnosis: Seminoma and testicular microlithiasis
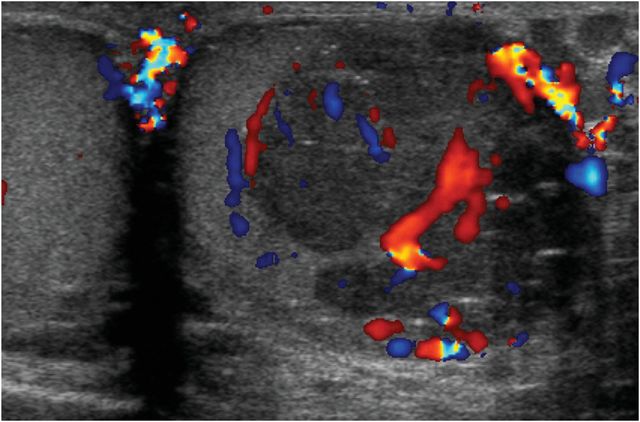
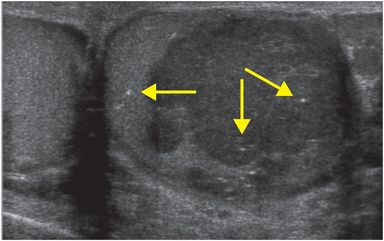
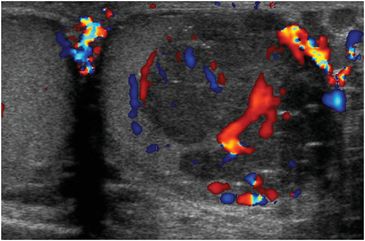
Grayscale and color Doppler ultrasound demonstrate a large, solid, lobulated, hypoechoic, left testicular mass, which demonstrates internal vascularity. Small specular reflectors within the mass and within the normal parenchyma represent microlithiasis (arrows).
Discussion
Primary testicular tumors are the most common malignancy in young adult males.
Testicular neoplasms commonly present as painless testicular enlargement or palpable scrotal masses.
Germ cell tumors account for 95% of testicular masses, and are usually malignant.
The most common germ cell tumor in adults is seminoma, which usually presents between 30 and 45 years of age.
Nonseminomatous germ cell tumor (NSGCT) subtypes include choriocarcinoma, teratoma, yolk sac tumor, embryonal cell carcinoma, and mixed germ cell tumor. Serum markers such as alpha-fetoprotein (AFP), lactate dehydrogenase (LDH), and the beta subunit of human chorionic gonadotropin (β-hCG) are elevated in patients with different tumor subtypes.
Seminomas are less aggressive than NSGCT, and are usually confined within the tunica albuginea at the time of diagnosis. They are highly radiosensitive and chemosensitive, hence their better prognosis.
Lymphoma and leukemia commonly involve the testis, and should be strongly considered in older patients with testicular masses, especially if bilateral.
Metastasis should be considered in patients with a known primary malignancy.
Uncommonly, intra-testicular masses may be benign: benign adrenal rests occur in patients with congenital adrenal hyperplasia, and sarcoidosis may affect the testes as well.
Ultrasound is the test of choice for the diagnosis of testicular neoplasm, with sensitivity near 100%. CT is used to evaluate for metastasis, usually to retroperitoneal lymph nodes.
Most testicular neoplasms are hypoechoic and hypervascular relative to the normal testicular parenchyma.
Ultrasound cannot definitively differentiate among types of testicular germ cell tumor; however, seminomas are generally homogeneous, while NSGCT are heterogeneous, with cystic areas and calcification.
Non-neoplastic testicular lesions that can potentially be confused with tumors, such as hematomas, abscesses, and infarcts, are differentiated from neoplasms by lack of internal vascularity.
Microlithiasis is an uncommon condition caused by calcification of collagenous material within the seminiferous tubules.
The testicular ultrasound criterion for diagnosis is five or more echogenic foci within the testicular parenchyma on a single field of view.
The strength of the association between testicular microlithiasis and malignancy is controversial, as the prevalence of microlithiasis in asymptomatic patients is unknown.
In a recent meta-analysis, Tan et al. demonstrated that asymptomatic patients in whom microlithiasis was incidentally detected had a low absolute risk of malignancy, while the summary risk ratio was 8.5-fold higher in patients with risk factors such as cryptorchidism (which raises risk of testicular neoplasm by about 30-fold), subfertility, or personal history of germ cell tumor.
Clinical synopsis
CT of the chest, abdomen, and pelvis demonstrated no metastatic disease. The patient underwent left radical orchiectomy, and histopathology was consistent with seminoma. Radiotherapy was followed by routine surveillance, which, to date, has shown no disease recurrence.
Self-assessment
|
|
|
|
|
|
Related posts:
 12 68-year-old man with left lower quadrant pain and hypotension
12 68-year-old man with left lower quadrant pain and hypotension
 72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
 35 37-year-old woman with a history of rheumatoid arthritis presenting with non-resolving bilateral effusions and chest pain
35 37-year-old woman with a history of rheumatoid arthritis presenting with non-resolving bilateral effusions and chest pain
 29 19-year-old male presented with acute onset right scrotal pain
29 19-year-old male presented with acute onset right scrotal pain
 53 42-year-old female presenting with fever and back pain
53 42-year-old female presenting with fever and back pain
 66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


