29.1 Introduction
This chapter focuses on the basic components, functions, and properties of display technology that are relevant to human perception and the conduct of medical image perception studies. Relevant aspects of liquid crystal displays (LCDs: the most commonly used in medical imaging) and organic light-emitting diode (LED) displays (an emerging display technology in the handheld and other niche markets) are summarized. Strengths and considerations of various display technology are outlined as they are available today. Basic information and guidance are provided in choosing and maintaining display technology to achieve performance recommendations for medical image viewing. Knowledge of these considerations is important for medical image perception studies as they impact the quality of the displayed image and hence observer performance.
29.1.1 Display Technology
The process of digital image display involves converting a digital signal from image pixel values into an array of light output. The imaging chain includes graphics cards, cabling, and the display itself, along with any tools used for maintaining the performance of the display.
The primary technology on the market for medical image display is the LCD. Organic LED (OLED) displays are emerging in the general consumer market, and may be found for medical image viewing with handheld devices. However, significant challenges remain to be addressed in display standards and/or in the OLED technology to provide for consistent image presentation in a diagnostic imaging chain that includes OLED displays.
29.1.1.1 Liquid Crystal Displays
The LCD creates an image through a matrix of polarized “shutters” through which light can pass with various levels of attenuation. The brightest pixels pass the most light and the dimmest or blackest pixels block the most light. The ability to independently modify the attenuation of each “shutter” relies on the properties of the liquid crystal (LC) that gives the display its name. The components of the LCD are shown in Figure 29.1.

Figure 29.1 The basic components of the liquid crystal display. Display model-dependent components are listed in square brackets. TFT, thin-film transistor.
LCD panel illumination comes from the combination of light sources and a diffuser panel. The light source for the display is called its backlight. Some LCDs still on the market use cold-cathode fluorescent lamps (CCFL) for their light source, either at the edge or as an array. More recently, the light sources have been replaced by LED bulbs that are more energy-efficient, have more stable light output, and can be longer-lived. In either case, the light sources are backed by a reflective layer and require a diffuser panel to create a uniform sheet of illumination for the LCD panel.
Variable light attenuation, needed to create the many grayscales of a medical image, is created by an LC layer sandwiched between polarizers. Light incident on the LC layer first passes through a polarization filter (Figure 29.1). The LC molecules rotate the polarization of the light passing through it, and the amount of rotation determines how much of the backlight passes through the front polarizer. The alignment of the LC molecules affects how the light is polarized.
The alignment of LC molecules is governed by grooves in their surrounding plates and applied local electric fields. When no electric field is applied the grooves govern alignment. Application of a local electric field (created from voltages applied to pixel electrodes) rotates the orientation of the LC molecules, shifting the LC cell between transmitting and blocking light. This effect is shown for one type of LCD panel in Figure 29.2, where the light transmission from the LC cell changes with the applied voltage across the pixel electrodes.

Figure 29.2 Curve describing a general relationship between light transmission from a liquid crystal display and the applied voltage to a liquid crystal cell, shown for the “normal white” type of display.
To create an image, the LC layer is divided into separately addressable pixels, each with its own tunable voltage. This is accomplished using a thin-film transistor (TFT) array that separately addresses the electrodes for each LC cell to create a pixel. Because the TFT element of each pixel does not transmit light, nor do the data lines or storage capacitors charged by the TFT, the smaller the pixel, the less area is available to transmit light (the light aperture), resulting in less light output at the display front panel.
There are different types of TFTs that are utilized for displays (both for LCD and OLED displays) that differ in their response times and efficiency. TFT array types being used for displays include: amorphous-silicon (a:Si-H), low-temperature polycrystalline silicon (LTPS), and indium gallium zinc oxide (IGZO) or other metal oxides. Amorphous-silicon panels are the most mature, most common, lowest-cost, and are what you will likely find with LCD workstation monitors. LTPS TFTs that permit higher pixel density may be found with some handheld LCD or OLED displays. IGZO and other metal oxide TFT arrays, which promise higher efficiency along with the higher pixel density, are beginning to be used more, particularly for mobile displays where high pixel density and lower power consumption are at issue (Hsieh, 2016).
Different types of LCD panels use different strategies for applying the electric field within each cell and the “electric-field off” orientation of the LC molecules. In-plane switching (IPS) LCDs have the electrodes that create the local field in the same plane (instead of on either side of the LC layer), improving the display viewing angle. Vertical alignment (VA) LCDs have LC molecules aligned perpendicular to the substrate, providing near-perfect blockage of light with cross-polarizers, and a resulting higher contrast ratio (Badano and Fifadara, 2004; Elze and Tanner, 2012).
In typical LCD panel structures, three or more subpixels are combined to one viewed pixel using a variety of subpixel arrangements (Yamazaki, 2013). For a monochromatic display, the multiple subpixels can allow for the possibility of greater grayscale resolution. For a color display, each TFT array subpixel has a color filter (typically RGB – red, green, blue) in front of it. By combining variations in RGB subpixel light output, one can vary the overall color of each pixel. Three 8-bit subpixels can represent a 24-bit color gamut (a “true-color” image).
29.1.2 Organic Light-Emitting Diode Displays
The OLED display (Figure 29.3) creates an image with a matrix of organic LEDs. Compared to the LCD, the OLED does not require a backlight, as each pixel is its own light source. It also uses a TFT array to separately address pixels. The TFT array is used to create the driving current for the OLED, with LTPS and metal oxide-type TFT arrays able to provide sufficient current for the OLED.
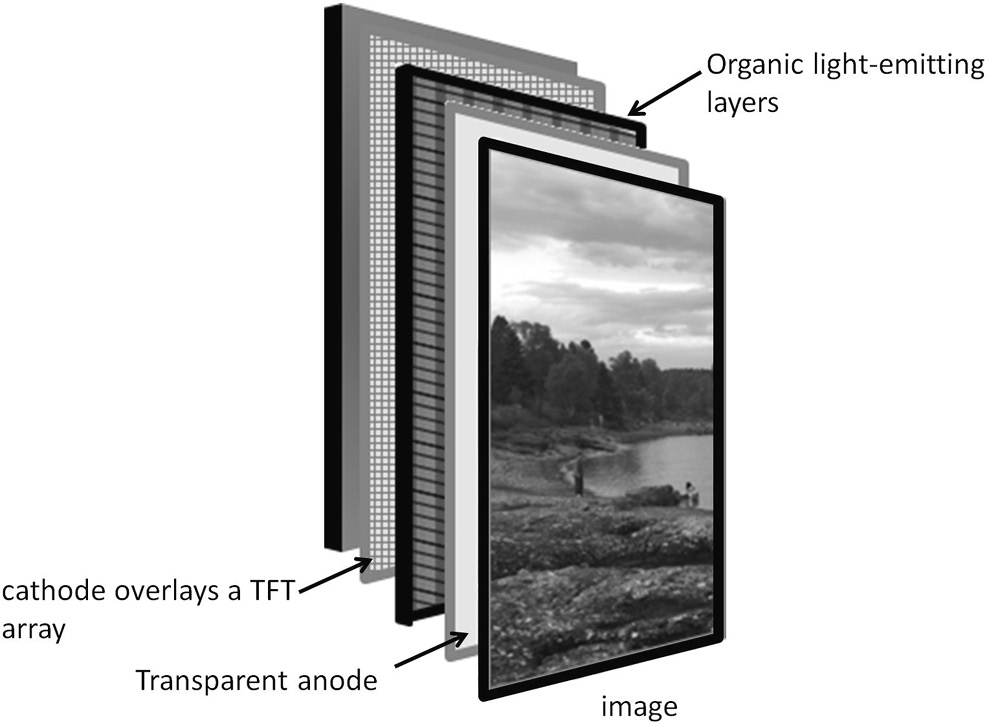
Figure 29.3 Basic components of a red, green, blue organic light-emitting diode display. TFT, thin-film transistor.
Like LCDs, OLED displays utilize subpixels to cover the color gamut used in the image display. Most of the OLED displays on the market use some combination of RGB or RGBW (W = white) subpixels that may be arranged in a variety of configurations (Yamazaki, 2013). Some OLED displays, called WOLEDs (white OLED displays) use white subpixels with color filters similar to the LCD configuration.
When current is supplied to the OLED pixel, light is emitted. When the current is off, no light is emitted. This means that OLED displays can have much higher luminance ratios than LCDs. They can require less power than LCDs with only the emitting pixels drawing power, and less light lost to filters. At present, OLED displays are found primarily in handheld device displays and in a growing television market. There are very few OLED workstation monitors on the market, only one that is independently marketed for medical image viewing, and none currently sold for diagnostic image viewing (as of November 2017). Outside of the challenge of supplying a niche market with high-resolution and high-bright panels in the desired form factor, there are some issues with image retention and luminance uniformity and stability that remain to be addressed before we may see OLED displays widely adopted for medical image viewing.
29.2 Graphics Controllers and Connectors
Graphics controllers, often called a graphics card, video card, or graphics processing unit, work by converting image data from the computer into a signal readable by the display device. It is important to select the appropriate graphics controller properties that are compatible with the computer, the display, and the imaging software. An appropriate graphics controller choice should render any large image files to full-fidelity, with the speed that is demanded by the user and can be provided by the software and display. For optimal resolution and performance it is necessary for the display and the graphics controller to be configured with compatible settings, with the graphics controller device driver set to the native resolution of the display. Software and display manufacturers will typically provide specifications for graphics controller requirements. Details that are of concern when selecting graphics controllers are how they connect to the computer (slot-type), how they connect to the display (cabling), bit depth, memory, and clock rate.
Some workstations utilize the graphics controller that is integrated on the same chip as the computer’s central processing unit (CPU). Integrated graphics controllers share computer system memory with all other applications. When the integrated graphics are insufficient for the needs of the display, software, or viewer, a dedicated (or discrete) graphics card can be used, connected to a computer’s motherboard through an expansion slot. Discrete graphics cards have their own memory. Different graphics controller–CPU connections (slot-type) offer different data transfer rates and bandwidths. Expansion slots come in different types, with the current standard being PCI-Express. PCI-Express cards come in different varieties (×1, ×4, ×8, and ×16), each utilizing a different number of pins and correspondingly having different bandwidths.
The graphics controller memory determines the limit for what image size and number of images can be loaded or manipulated for delivery to the display. This works with the clock rate in determining the overall speed performance of display graphics rendering. Displays capable of using 10 bits per RGB color channel will need a graphics controller that supports that. The display connector must be compatible with the monitor inputs and different connectors allow for different bit depths and refresh rates. Digital-only connectors should be used, avoiding analogue connectors like video graphics array (VGA).
There are three main types of digital display connectors currently available: DVI-D, HDMI, and DisplayPort. DVI-D comes in two types: single-link and dual-link. Dual-link is needed for higher-resolution monitors, and has extra pins that can support higher data rates. A dual-link DVI-D cable can run a 2560 × 1600 display at 60 Hz. DisplayPort can handle larger displays at higher refresh rates. Table 29.1 shows the data rates for various cable versions.
Table 29.1 Maximum data rate for various cable types and versions
| Cable type and version | Maximum data rate (Gb/s) | Maximum pixel array at 60 Hz with true color (24 b/pixel) |
|---|---|---|
| DVI-D single-link | 4.95 | 1920 × 1200 |
| DVI-D dual-link | 9.9 | 2560 × 1600 |
| HDMI 1.4 | 8.6 | 2560 × 1440 |
| HDMI 2.0 | 14.4 | 3840 × 2160 (4K) |
| DisplayPort 1.1 | 8.6 | 2560 × 1440 |
| DisplayPort 1.2 | 17.3 | 3840 × 2160 (4K) |
| DisplayPort 1.3 | 25.92 | 5120 × 2880 (5K) |
| DisplayPort 1.41 | 25.92 | 7680 × 4320 (8K |
1 The capability of DisplayPort to run an 8K display at 60 Hz requires the use of data stream compression.
29.3 Tools for Display Assessment: Terminology and Equipment
29.3.1 Terminology
Display characterization involves measurement of light output or ambient light reflection in magnitude, spectral properties, and spatial or temporal variation. Before further exploring specific display properties, basic terms and concepts will be outlined to provide the reader with some basic concepts for how displays are characterized.
Luminous flux refers to visible light power output and is measured in lumens (lm). Equipment measuring in lumens (or related quantities) is calibrated to measure light power at wavelengths visible to the human eye, weighted by a luminosity function that represents the eye’s response to different wavelengths.
Luminous intensity refers to luminous flux (lm) per unit solid angle (sr). Luminous intensity is measured in candelas (cd).
Luminance refers to the amount of light power (lm) emitted in a given direction (per unit angle, sr) from a particular source area. It is measured in candelas/meter2 (cd/m2). Luminance is used to describe the measured light emitted or reflected from a display. This is the property that correlates to perceived display brightness. A typical computer display has a maximum luminance ranging from 200 to 500 cd/m2, while high bright medical image displays for mammography are designed for normal use with a maximum of 1000 cd/m2. The number of luminance values that a digital display can represent is given by the bit-depth of the system.
Illuminance refers to a magnitude of light power (luminous flux) hitting a particular area from all directions (many or distributed sources). This is the quantity used to characterize ambient light. Illuminance is measured in lux (lm/m2). Typical reading rooms are 10–60 lux.
Specular reflection is what people normally think of as reflection. It occurs when light incident on a surface is reflected in a particular direction, as for a shiny surface or a mirror. Displays with high specular reflection coefficients will look shinier.
Diffuse reflection occurs when light incident on a surface is broadly scattered. This contribution to measured or perceived luminance comes from reflection of surface illumination that is scattered over all angles from the surface. This is what we see when something looks bright when it is illuminated (like the moon, or a sheet of white paper), but does not look shiny. The magnitude of diffuse reflection is proportional to the illumination of the display from ambient light sources and the display’s diffuse reflection coefficient.
Color point or white point: The color properties (or chromaticity) of a display are characterized by its color point or white point (i.e., the color coordinates that describe “white”). Color or white points can be described as a two-dimensional coordinate in a CIE (International Commission on Illumination) chromaticity space such as (u’, v’) in the CIE 1976 LUV color space (CIE, 2004). A third coordinate, L’, of the CIE 1976 LUV color space represents the brightness.
29.3.2 Equipment for Measuring Display Characteristics
The primary tools used for assessing display properties include:
human visual system
high-resolution cameras
photometers and colorimeters.
Tests involving the human visual assessment of test patterns are core elements of display quality control in medical imaging. Visual tests are easily accessible and are most closely tied to a clinically relevant assessment. However, visual tests are subjective in nature, involving human perceptual factors which are the focus of Chapter 30. This chapter largely focuses on display characterization and maintenance with regard to quantitative evaluation that is not subject to visual interpretation.
Low-noise, high-resolution cameras are the measurement standard for quantitative display analysis involving spatial properties. Such measurements can be challenging and costly to perform, and are generally not practical for end-users. Descriptions of such tests are provided only in terms of referencing measurements done in research laboratories and not meant to be instructional for the reader in performing such tests.
Photometers are tools used to measure luminous flux and come in various configurations to enable measurement of luminance or illuminance. Colorimeters are photometers that are outfitted with color filters that allow for estimation of the color coordinates of the measured light.
To measure luminance, the light (luminous intensity) is constrained in a given direction from a source area, by either placing the photometer directly against the display (contact photometer) or using a baffle (spot photometer). Contact photometers (as shown in Figure 29.4) measure only display luminance, while spot photometers measure the sum of display luminance and luminance from reflected ambient light, and can be employed to measure luminance at different viewing angles. For either contact or spot photometers, care must be given to ensure that the area of capture corresponds with the desired area of measurement (i.e., the desired part of a test pattern).

Figure 29.4 Contact photometers for measuring luminance: (a) integrated front-panel photometer; (b) handheld photometer.
Displays sold for medical imaging often come with panel-integrated photometers that measure an area of display luminance near the edge of the display. These integrated photometers can be set to automatically calibrate or test the luminance of a display in off-hours without disturbing users or requiring in-person visits. Measurement results can be relayed to a quality control server that can be used to both configure testing and view the results. Because the photometer is integrated, it cannot be used to assess uniformity of luminance over the full display area.
To measure ambient light (or illuminance), photometers are outfitted with a diffuser to collect light from all directions incident on a surface. For most real-life situations the amount of incident light is highly dependent on the position and plane of measurement. Variability in illuminance gives rise to display calibration strategies that are robust to a range of ambient light.
Photometers using color filters are commonly referred to as colorimeters. Typically three separate filters are used to characterize the spectral properties of the light (chromaticity). Colorimeters are calibrated to measure chromaticity and brightness in terms of a point in a CIE color space. The CIE 1976 (L*, u*, v*) color space, also known as the CIELUV color space, is a commonly referred-to color space in colorimetry. Colorimeters may also provide outputs in terms of other CIE color spaces, related to each other through simple matrix transformations.
The accuracy of a photometer is determined by its calibration, traceable to a standard. Accuracy of a photometer varies depending on the luminance range, with many consumer-grade colorimeters showing high variability with low light (Badano et al., 2016). Like all measurement tools, photometers’ accuracy may drift and they should be recalibrated or checked against another calibrated photometer to ensure accuracy. Recommended frequencies for calibration or replacement may be provided by the manufacturer. Panel-integrated photometers that cannot be sent back for recalibration must be recalibrated or recorrelated by the end-user using another calibrated photometer. Multiple groups have shown that this re-correlation of an integrated photometer is needed over the typical lifetime of a display to retain the desired display calibration (Ruuge et al., 2016; Silosky and Marsh, 2013).
29.4 Display Factors that Impact Viewing and How They Relate to Technology Options and Utilization
29.4.1 Pixel Pitch, Viewing Distance, and Resolution
Consumers looking at specifications of pixel pitch for information about display resolution should be aware that display resolution also depends on other factors, including pixel structure (Yamazaki, 2013), and can be degraded by blurring or reflections caused by the display front panel (Eizo, 2015).
Objectively, the intrinsic resolution of a display resulting from these three factors (pixel pitch, viewing distance, resolution) is captured by measurements of its modulation transfer function (MTF). The MTF describes the system’s ability to reproduce different spatial frequencies (Bushberg, 2012). Measurement of the display’s MTF is described in the report from Task Group 18 of the American Association of Physicists in Medicine (AAPM) (Samei et al., 2005). MTF measurements require high-resolution charge-coupled device (CCD) cameras and are not practical or possible for most users, who might instead look to research laboratories for information on how pixel pitch, pixel structure, and panel properties might modify the resolution implied by the pixel pitch. In general, for the intended purpose of the displays, visual tests as described in Chapter 30 are sufficient for monitoring and comparison of displayed spatial resolution.
The displayed resolution of an image source will also depend on how the image is mapped to the display pixels (or sampled by the display graphics controller). The more pixels a display has (e.g., 2 MP, 3 MP or more) mean more of the source image can be displayed at higher resolution without zooming in. However, if there is not a one-to-one relationship between source image pixels and display pixels, the displayed resolution can also be degraded by how the image is mapped to the display. To mitigate potential interpolation artifacts, the graphics controller driver settings should match the native resolution of the display. Other suggestions for interpolation settings are described in the American College of Radiology (ACR)-AAPM-Society for Imaging Informatics in Medicine (SIIM) technical standard (ACR, 2017).
Measured or perceived resolution is also determined by measurement or viewing distance. A display with a 0.2-mm pixel pitch (2.5 line pairs/mm) represents 28 cycles per degree for a 65 cm viewing distance.1 To maintain the same measured or perceived resolution at a handheld distance of 30 cm the display pixel pitch would need to be 0.09 mm per pixel. For a viewing distance of 160 cm (as might be the case in a surgical or interventional suite) the equivalent pixel pitch would be 0.5 mm pixel pitch.
Since intrinsic spatial resolution of an LCD or OLED panel is fixed, spatial resolution is a stable property of the display and not a relevant factor in quality control for the display itself. However, changes in graphics card settings may induce interpolation artifacts that degrade spatial resolution. Thus, if system settings are not carefully controlled, the displayed image resolution could be changed and be a relevant aspect for display monitoring.
29.5 Luminance: Calibration and Stability
29.5.1 Luminance Calibration
To obtain consistency in image display, it is necessary to set and maintain a known displayed luminance for each pixel in response to a digital image signal (the digital driving level). The mapping between the digital driving level (DDL) and the luminance output is called the display look-up table (LUT). The LUT communicates the needed voltage or current to the display pixel to render the desired light output. The process of setting the desired relationship between pixel DDL and luminance output is what is referred to as display luminance calibration. For consistency in grayscale representation between displays, a calibration standard must be chosen and followed. The grayscale calibration standard currently utilized in medical image displays is known as the DICOM (Digital Imaging and Communications in Medicine) grayscale standard display function (GSDF), and is described in more detail in Chapter 30.
Since the digital display signal associated with each DDL is individually assigned, full characterization of the display luminance response, or validation of display response, requires measurement of each DDL (this is 256 values for an 8-bit grayscale display). Once an LCD panel is fully characterized, the most common source of change in luminance response for an LCD relates to age-related dimming of the backlight or other changes that are global in nature (affecting each DDL). Thus, it is possible to measure and calibrate a display by sampling a subset of DDLs, as is typically done for quality control of displays for medical image viewing. Often the 18-different luminance patterns provided by the AAPM Task Group 18 are utilized for the purpose of measuring and correcting calibration after it has been initially configured.
Software provided by the display manufacturer or other sources (Flynn, 2013) may be used to calibrate a display’s luminance response.
While only a small region of the display may be measured during calibration, if the display panel has uniform luminance and uniform response to changes in digital driving levels, then the whole panel will be appropriately calibrated. Issues may arise if nonuniformities in the panel develop from image sticking or nonuniform panel aging, in which case the calibration determined from one region of the display results in a different luminance response in a different part of the display. The display calibration is global and cannot fix the panel nonuniformity.
The display LUT may be stored on the display itself or with the graphics controller. Displays sold for medical imaging typically allow for LUTs to be stored by the display itself and will typically come pre-calibrated from the factory, with full characterization of each DDL. A graphics controller-based LUT is only an option if software can be loaded to enable it, or in the case of a multihead workstation, the graphics controller can store unique LUTs for each display. Keeping the LUT tied with the display can make it easier and less time consuming to ensure that the LUT has been appropriately set for the intended monitor. For a graphics controller-based LUT, if the display is swapped, or in the case of a multihead workstation, the cables are swapped between displays, you will need to recalibrate the display to get the appropriate LUT set for the desired luminance response. An LUT that is stored with the display allows for the display to be calibrated prior to deployment and can be useful in situations where the end-user is not able to load software on a workstation.
29.5.2 Maximum Luminance, Minimum Luminance, and Luminance Stability
The light output for a given DDL can change as a display warms up, over the course of operation, or because of the driving levels of other pixels (as is the case for OLED displays). It is important to understand how to select and manage equipment for stable operation if consistent image display is desired.
29.5.2.1 LCDs
Currently all of the displays on the market for diagnostic image viewing utilize LCD panels (Mertens, 2017). LCD panels sold for medical imaging are generally well characterized, demonstrating good, stable performance over the warranted lifetime of the display.
The maximum luminance from an LCD display is governed by how much of the backlight is transmitted. To have a stable maximum luminance output, either the backlight must be stabilized or the LCD panel must be recalibrated to adjust for changes in backlight. LCDs sold for medical imaging have two features that allow for their light output to be stable over time: higher-luminance backlights and backlight stabilization. Typical backlights in LCDs sold for medical imaging are capable of producing more light output than is needed to produce the desired maximum luminance (i.e., the “calibrated” maximum). This allows the display to compensate for age-related backlight dimming by driving the backlight harder to boost its luminance output. In addition, displays for medical image viewing typically have backlight stabilization circuitry that measures the output from the backlight with an internal photometer and provides compensating drive to maintain a stable output. This stabilization can help with quickly achieving stable output after the display is turned on, keeping it stable for hours, weeks, and months of operation.
Figure 29.5 shows the short-term luminance behavior for displays with unstabilized and stabilized backlight as well as with CCFL and LED backlights. LED backlights can have a faster response time and potentially longer life (range of luminance stability) and are more efficient than CCFL, making them the preferred choice for new LCD models. In addition, LCDs without stabilized backlights may show different luminance output decay behavior, despite having the same starting value, as shown for a pair of the same older model display in Figure 29.6. Variation in luminance over time can create difficulties for quality control, when measurements vary depending on the length of time that the display has been on.

Figure 29.5 Measured maximum luminance as a percentage of the maximum calibrated luminance for a liquid crystal display with stabilized and nonstabilized cold-cathode fluorescent lamp (CCFL) backlights. LED, light-emitting diode.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


