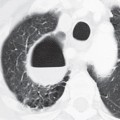
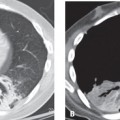
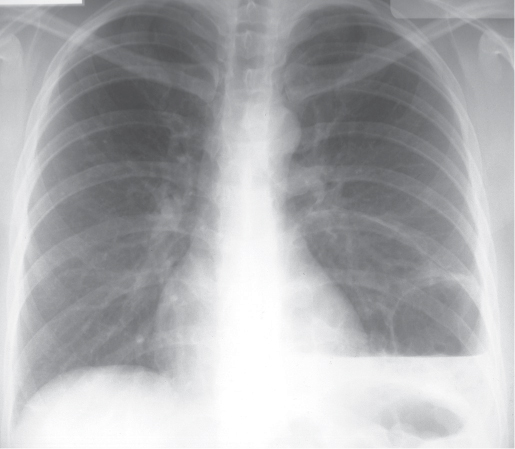
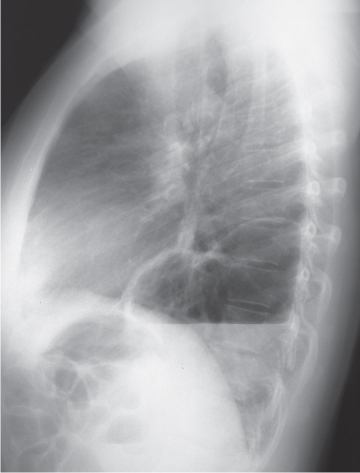
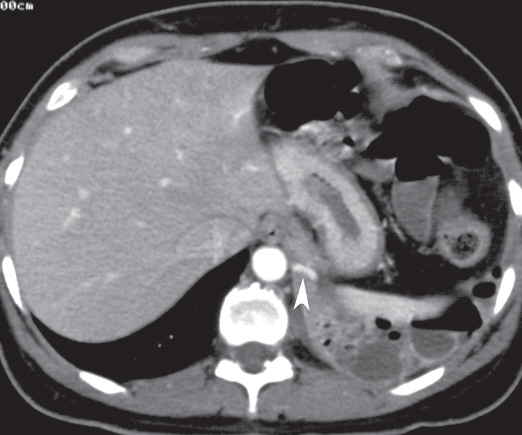
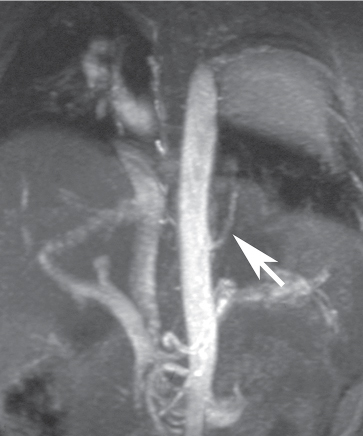
CASE 3 37-year-old woman with recurrent pneumonia and productive cough PA (Fig. 3.1) and lateral (Fig. 3.2) chest radiographs demonstrate a left lower lobe thin-walled multilocular cystic lesion with a large air-fluid level. Contrast-enhanced chest CT (mediastinal window) (Fig. 3.3) through the inferior chest demonstrates a heterogeneously enhancing left lower lobe lesion with soft tissue, air, and fluid attenuation components, supplied by a branch of the descending thoracic aorta (arrowhead). Coronal gradient-echo MRA (Fig. 3.4) demonstrates the aortic arterial branch (arrow) that supplies the lesion. Intralobar Sequestration • Pneumonia (including post-obstructive pneumonia from central obstruction) • Lung Abscess • Bronchiectasis (with secondary infection) • Infected Bullae Fig. 3.1 Fig. 3.2 Fig. 3.3 Fig. 3.4 The term pulmonary sequestration refers to lung parenchyma that does not communicate normally with the tracheobronchial tree and has a systemic blood supply. Intralobar sequestrations are four times more frequent than extralobar sequestrations and occur almost exclusively in the lower lobes, slightly more frequently on the left. The systemic arterial supply to the lesion often courses within the pulmonary ligament and typically originates from the descending aorta, although other systemic arteries (abdominal aorta, inferior phrenic, coronary) may participate. The venous drainage is typically (95%) normal into the pulmonary veins. The lesion is often heterogeneous due to acute and chronic inflammation and bronchopneumonia with resultant bronchiectasis, fibrosis, and cystic change. The lesion typically abuts adjacent normal (nonsequestered) lung. Extralobar sequestrations represent accessory pulmonary lobes that result from abnormal foregut budding and are located outside the confines of normal lung. They may occur in the thorax, diaphragm, or abdomen; are characteristically supplied and drained by the systemic circulation; and represent true congenital anomalies. Affected patients are typically diagnosed within the first 6 months of life, but a small number of lesions (10%) are diagnosed in asymptomatic adults.
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Etiology
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Radiology Key
Fastest Radiology Insight Engine