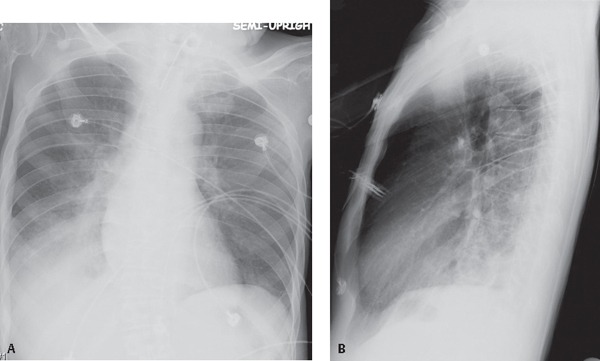
CASE 53 28-year-old quadriplegic ventilator-dependent man with fever, chills, and purulent sputum production PA (Fig. 53.1A) and lateral (Fig. 53.1B) chest X-rays demonstrate non-segmental right lower lobe consolidation without associated volume loss and an ipsilateral pleural effusion. Note the tracheostomy device. Sputum and blood cultures confirmed the diagnosis. Pseudomonas Pneumonia • Staphylococcus aureus • Group A Streptococci • Klebsiella pneumoniae Fig. 53.1 • Escherichia coli • Proteus sp. • Enterobacter • Serratia marcescens Pseudomonas may cause either bacteremic or non-bacteremic pneumonia. Bacteremic infection is acquired through breaks in the skin, the gastrointestinal mucosa, or respiratory tract, and most often occurs in patients with underlying hematologic or lymphoreticular malignancies, HIV-AIDS, immunosuppression, neutropenia, debilitation, or severe burns. Non-bacteremic infection is usually acquired through aspiration of infected oropharyngeal secretions. Risk factors for non-bacteremic Pseudomonas infection include advanced age, debilitation, chronic cardiopulmonary disease, COPD patients receiving steroids, cystic fibrosis, diffuse panbronchiolitis, and contaminated respiratory therapy equipment. Pseudomonas sp. is ubiquitous and survives in water, vegetation, and soil. Infection may result from exposure to contaminated hot tubs, whirlpools, vegetables, flowers, nails, and splinters. Because of resistance to many disinfectants, it is a common cause of nosocomial infection. In fact, P. aeruginosa
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
Community-Acquired Pneumonia
Opportunistic Pneumonia
 Discussion
Discussion
Background
Etiology
![]()
Stay updated, free articles. Join our Telegram channel





Full access? Get Clinical Tree


