
Diagnosis: Esophageal rupture post upper endoscopy
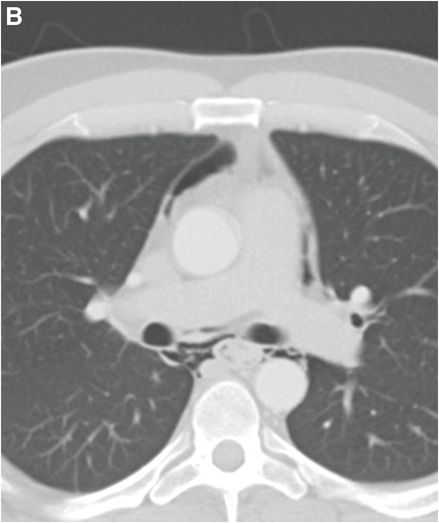
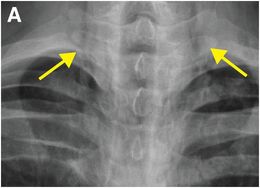
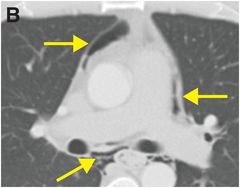
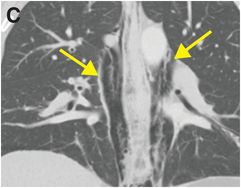
Chest radiograph (A) demonstrates streaky lucencies outlining the mediastinum, most prominently seen extending to the lower neck (arrows), consistent with pneumomediastinum. Axial (B) and coronal (C) enhanced CT images confirm the presence of extensive pneumomediastinum (arrows), with a large amount of air surrounding the esophagus. No direct esophageal injury is identified.
Discussion
Overview and etiology of esophageal rupture
The esophagus is more prone to rupture in comparison to other hollow viscera due to its lack of supporting adventitia and relatively poor blood supply.
Iatrogenic perforation is the most common cause of esophageal rupture, which may occur as a complication of upper endoscopy or more invasive surgical procedures. An impacted food bolus may also cause esophageal rupture due to pressure necrosis. Other etiologies of esophageal rupture include malignancy, trauma, esophagitis (infectious, reflux, post radiation), and increased intraluminal pressure (Mallory–Weiss tear).
The symptoms of esophageal injury (and rupture) are nonspecific, including severe chest pain, dysphagia, and odynophagia.
Imaging of esophageal injury
Although a water-soluble contrast esophagram is considered the imaging modality of choice for suspected esophageal injury, CT is most often performed due to immediate availability and ability to identify alternative diagnoses for a nonspecific clinical presentation. If esophageal injury is clinically suspected, water-soluble oral contrast can be helpful.
On CT imaging, pneumomediastinum is almost always seen in the setting of esophageal rupture, even in the absence of direct visualization of an esophageal defect, as in the case above. However, it is important to note that although pneumomediastinum can be the result of esophageal rupture, alveolar rupture due to barotrauma is overall the most common cause of pneumomediastinum. Pneumomediastinum as an isolated finding is nonspecific and may also occur in patients with asthma, during straining against a closed glottis (parturition, weight lifting, vomiting), after blunt chest trauma, or due to traumatic airway laceration.
Other CT findings of esophageal injury include direct visualization of a mural defect, extravasation of oral contrast, and periesophageal gas and/or fluid collections. Ancillary signs of esophageal injury include mediastinal fat stranding and pleural effusion.
Related posts:
 12 68-year-old man with left lower quadrant pain and hypotension
12 68-year-old man with left lower quadrant pain and hypotension
 72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
 28 30-year-old male presented with a palpable left testicular mass
28 30-year-old male presented with a palpable left testicular mass
 29 19-year-old male presented with acute onset right scrotal pain
29 19-year-old male presented with acute onset right scrotal pain
 53 42-year-old female presenting with fever and back pain
53 42-year-old female presenting with fever and back pain
 66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


