Diagnosis: Empyema
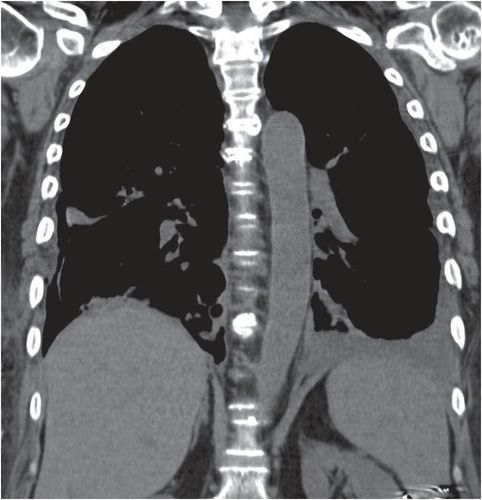
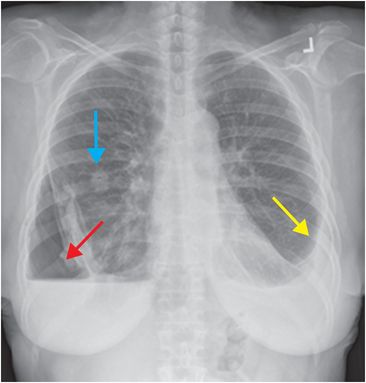
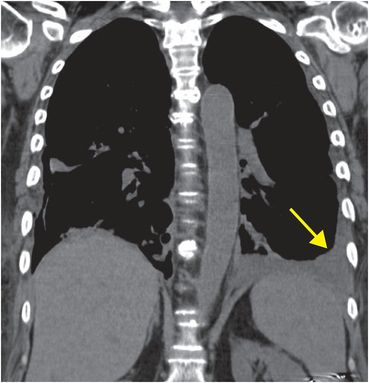
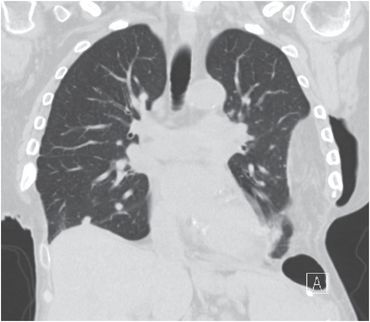
Frontal chest radiograph demonstrates a left pleural effusion (yellow arrow) and a right hydropneumothorax (red arrow). A right-sided lung nodule is present (blue arrow). Coronal noncontrast CT image better demonstrates the complex left pleural effusion with associated pleural thickening (yellow arrow). Diagnostic thoracentesis confirmed that the effusions were infected.
Discussion
Empyema is defined as an infected pleural effusion or collection. There are three stages in the evolution of empyema.
The first or “exudative” stage is characterized by rapid egress of fluid from the pulmonary interstitial space into the pleural space, which may be augmented by capillary leakage. Evaluation of pleural fluid indicates that the effusion is exudative rather than transudative by Light’s criteria, but bacterial cultures are negative.
Without appropriate treatment, there is progression to the second or “fibropurulent stage”, in which the pleural fluid becomes infected and loculated.
If the collection is not drained, progression to the third stage, the development of a thick “pleural peel,” may occur due to transit of fibroblasts from the parietal and visceral pleura into the empyema. This pleural peel may restrict lung movement and must be surgically removed (decorticated) by open thoracotomy or video-assisted thorascopic surgery (VATS).
Empyema is defined as an infected pleural effusion or collection. There are three stages in the evolution of empyema.
Empyema appears as a loculated effusion with a lenticular appearance.
CT can be used for confirmation and assessment for underlying pneumonia.
CT is also the best modality for identification and characterization of complications such as bronchopleural fistula (BPF) and empyema necessitans, defined as extension of the pleural collection out of the pleural space into the chest wall.
When clinical features and imaging suggest the diagnosis, diagnostic thoracentesis is performed.
Empyemas are treated with aggressive antibiotics.
Surgical decortication may be helpful in patients who do not respond to antibiotics or in cases of moderate or large empyema, and may include a Clagett window procedure. In the Clagett window procedure, a small thoracotomy is left open for ongoing irrigation with antibiotic solution and drainage. When infection has resolved and granulation tissue has formed, antibiotic solution is instilled into the pleural space and the window may be closed using muscular flaps from the latissimus dorsi.
Clinical synopsis
The bilateral empyemas did not resolve even after repeated courses of aggressive intravenous antibiotics. The right pneumothorax was caused by previous thoracentesis attempt, and the right-sided lung nodule was thought to be a rheumatoid necrobiotic nodule. The patient underwent bilateral surgical decortication and creation of Clagett windows. Upon resolution of infection, closure was achieved with bilateral latissimus dorsi flaps.
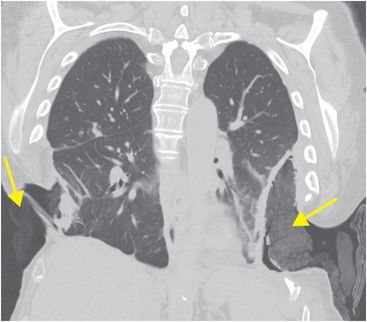
Noncontrast CT image of the chest in the coronal plane (left image) shows bilateral Clagett windows, which provide communication between the pleural space and the outside. Mixed density packing material is visible (arrows). After resolution of infection, repeat noncontrast coronal CT shows that the Clagett windows have been closed with latissimus dorsi flaps.
Self-assessment
|
|
|
|
|
|
Related posts:
 12 68-year-old man with left lower quadrant pain and hypotension
12 68-year-old man with left lower quadrant pain and hypotension
 72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
 28 30-year-old male presented with a palpable left testicular mass
28 30-year-old male presented with a palpable left testicular mass
 29 19-year-old male presented with acute onset right scrotal pain
29 19-year-old male presented with acute onset right scrotal pain
 53 42-year-old female presenting with fever and back pain
53 42-year-old female presenting with fever and back pain
 66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


