CASE 36 A 7-year-old was referred for suspected tuberculosis based on the provided chest radiograph. Figure 36A Figure 36B Frontal (Fig. 36A1) and lateral (Fig. 36A2) chest radiographs show left hilar enlargement, resembling adenopathy. The lateral view shows a well-defined density. Axial enhanced CT images (Fig. 36B) demonstrate a round, nonenhancing mass posterior to the left hilum, which is consistent with the typical appearance of a bronchogenic cyst. Bronchogenic cyst Bronchogenic cysts are thought to arise when a small bud of the developing tracheobronchial tree becomes amputated and isolated. These cysts may occur in the mediastinum or in the lung parenchyma. Mediastinal cysts are usually located near the carina, behind the trachea, or along the mainstem bronchi. The intrapulmonary bronchogenic cysts appear as solitary round or oval thin-walled, air-containing cysts. Bronchogenic cysts are usually isolated and, in the uncomplicated state, do not communicate with the tracheobronchial tree. Bronchogenic cysts usually do not present in infancy. It is estimated that over half of these cysts will present after 15 years of age. Most lesions that present in infancy do so by their mass effect on regional structures, whereas most (95%) that present after infancy do so by becoming infected.
Clinical Presentation
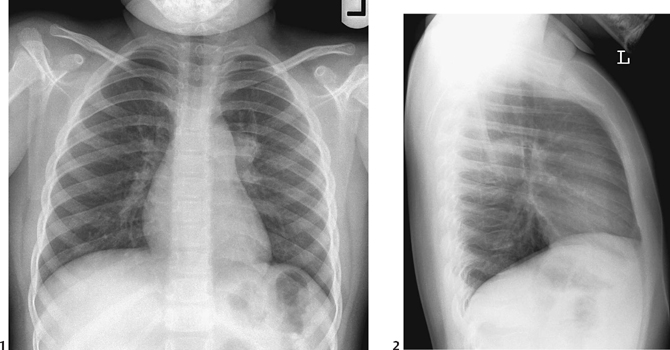
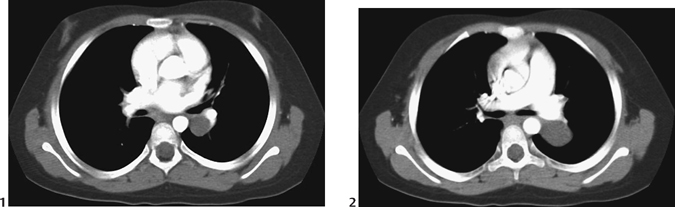
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Etiology
Histology
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


