36 Renal Cyst
36.1 Case Presentation
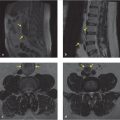
A 71-year-old man presents with lower back pain. An MRI of the lumbar spine without contrast was performed to evaluate for radiculopathy (▶ Fig. 36.1; also see ▶ Table 36.1).

36.2 Diagnostic Testing Needed
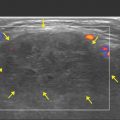
When renal cysts are identified in lumbar spine MRI without contrast, they may be further evaluated with renal ultrasound, or renal mass protocol CT/MR, depending on their complexity and size. Ideally, if prior imaging is available, comparison can be helpful to determine stability versus changes. Fluid density cysts that are T2 hyperintense and T1 hypointense are most certainly benign and require no further follow-up especially if these are less than 1 cm, and follow fluid signal like cerebrospinal fluid (CSF) on T2 and T1 sequences, 5 have no solid components, and have well-defined borders. Fluid density cysts greater than 1 cm or those lesions that are partially imaged can be evaluated by renal ultrasound. Lesions without fluid signal or lesions on MRI that are greater than 1 cm can be evaluated by CT/MR renal mass protocol. 5 , 6
On nonenhanced CT, homogenous lesions with internal attenuation less than 20 HU (simple cyst) or greater than 70 HU (hemorrhagic cysts) are considered benign and require no further follow-up, but if the lesions have internal attenuation of between 20 and 70 HU, they are deemed indeterminate and require further workup. 7 , 8 Studies have shown that homogeneous renal lesions greater than 70 HU on nonenhanced CT have a greater than 99.9% of being a hemorrhagic cyst than renal cell carcinoma. 9 This is pertinent as renal cysts can be seen on noncontrast CT of the lumbar spine.
Because the patient had a history of treated lung cancer, a PET/CT was performed to evaluate for the presence of residual disease and a CT abdomen and pelvis with contrast was performed for abdominal pain. Typically, PET/CT examinations are not performed to evaluate renal cysts, but in our patient’s case, the PET/CT examination was useful because it allowed for comparison of the renal cysts. Therefore, the left renal cysts seen on this MRI study can then be compared to these studies.
Given that the left inferomedial cyst was hyperdense in the noncontrast image (white arrow in ▶ Fig. 36.2a) and was T1 hyperintense and T2 hypointense, this structure is most likely a proteinaceous/hemorrhagic cyst and requires no further follow-up. Similarly, the T2 hyperintense and T1 hypointense nonenhancing fluid density inferoposterior cyst is a simple cyst, and requires no further follow-up.

Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


