38 Adrenal Mass
38.1 Case 1
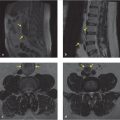
A 77-year-old woman presents with pain in the thoracic spine and left lower quadrant abdominal pain. MRI of the thoracic spine was performed to evaluate the etiology of back pain (▶ Fig. 38.1).

38.1.1 Imaging Impression
Incidentally detected, right adrenal lesion on MRI, incompletely evaluated, and remains indeterminate.
38.1.2 Additional Testing Needed
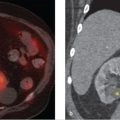
A CT adrenal mass protocol consisting of precontrast, enhanced, and delayed phases is needed for complete evaluation of the right adrenal lesion, where the absolute washout of the adrenal lesion can be calculated. Alternatively, chemical shift MR sequences can also be formed to evaluate for the presence of microscopic fat in the adrenal lesion, with signal loss in the opposed-phase images. In our case, the clinician ordered a CT adrenal mass protocol to evaluate the right adrenal lesion (▶ Fig. 38.2).

38.1.3 Imaging Impression
The right adrenal nodule showed an attenuation of 5 HU in the precontrast image, 65 HU in the portal venous phase, and 25 HU in the delayed phase, and has a calculated absolute washout of 66.6%, consistent with a lipid-rich adenoma (please see formula below for absolute washout calculation). Indeed, when an adrenal lesion shows an attenuation of less than 10 HU in the precontrast phase, this finding has a greater than 98% specificity that the lesion is a lipid-rich adrenal adenoma, and in this case, a precontrast image would have been sufficient to diagnose the right adrenal lesion as a lipid-rich adenoma.
However, should an adrenal nodule show an attenuation of greater than 10 HU on the precontrast phase, the lesion is considered indeterminate, as there is overlap between a lipid-poor adenoma (about 30% of all adenomas) with other more sinister adrenal lesions like malignancy, metastases, and pheochromocytomas. In such an instance, a CT adrenal mass protocol is then performed, which consists of a precontrast, 1-minute (post) postcontrast, and 15-minute delayed (delay) phase used to ascertain if that adrenal lesion demonstrates washout kinetics characteristic of an adenoma. Adrenal washout can either be calculated as absolute percentage washout (APW) or as relative percentage washout (RPW) if only enhanced and delayed CT images are available. The formulas for absolute washout (APW) and relative washout (RPW) are as follows:

For example, if the absolute washout is greater than 60%, then this classifies the adrenal lesion as a benign adenoma. If the relative washout is greater than 40%, then this classifies the adrenal lesion as a benign adenoma.
Alternatively, a chemical shift MR protocol utilizing T1-weighted in- and opposed-phase imaging can also be performed to look for microscopic fat in the adrenal lesion. A region of interest is selected over the adrenal lesion and the arbitrary attenuation units compared between the in- and opposed-phase images. A loss of signal greater than 20% in the opposed-phase image would indicate the presence of microscopic fat in the adrenal nodule, consistent with a lipid-rich adenoma. In the event that the chemical shift MR method is inconclusive, a CT adrenal mass protocol should be performed to allow better quantification.
Management: No further imaging is required for this adrenal adenoma. As there was no clinical evidence of adrenal hyperfunction, this patient was diagnosed with an incidentally detected, nonfunctioning adrenal adenoma.
38.2 Case 2
A 76-year-old man presents with low back pain extending to the right side. MRI of the lumbar spine was performed to investigate the etiology of patient’s back pain (▶ Fig. 38.3).

38.2.1 Imaging Impression
Incidentally identified left adrenal lesion with high T2 signal, suggestive of fluid component but not conclusive.
38.2.2 Additional Testing Needed
A CT abdomen and pelvis with contrast was performed to evaluate the left adrenal lesion (▶ Fig. 38.4).

38.2.3 Imaging Impression
The finding of an adrenal lesion with high T2 signal is not diagnostic of an adrenal cyst as a pheochromocytoma can also have high T2 signal. However, a CT with contrast demonstrates fluid density and no enhancement of an adrenal lesion is consistent with an adrenal cyst, requiring no further follow-up. In the case of a pheochromocytoma, the patient may be symptomatic, demonstrate high levels of metanephrines in the urine, and on imaging will show enhancement on contrast CT/MR, unlike the lack of enhancement in an adrenal cyst.
Management: Benign adrenal cyst requiring no further follow-up or workup.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


