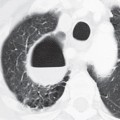
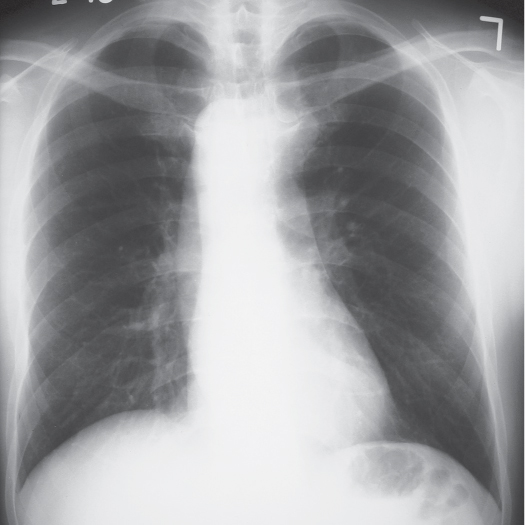
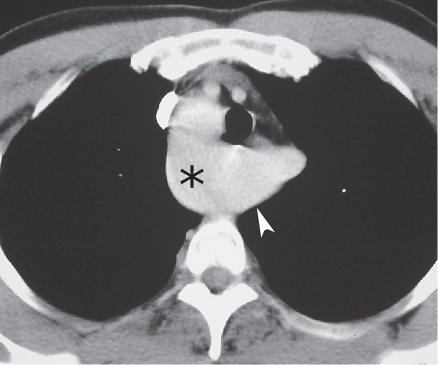
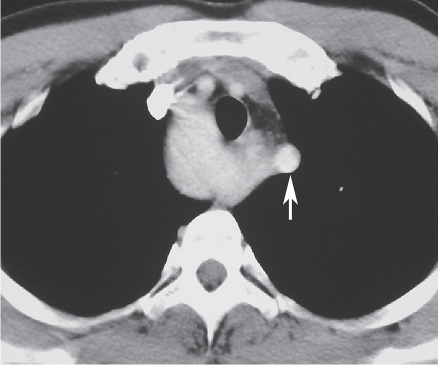
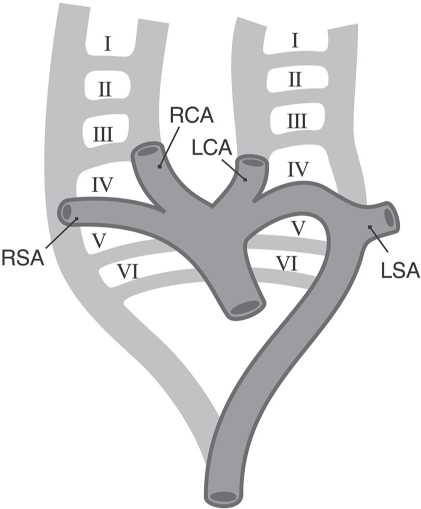
CASE 4 43-year-old man evaluated prior to neck surgery PA (Fig. 4.1) chest radiograph demonstrates a right-sided aortic arch with a right descending aorta. Contrast-enhanced chest CT (mediastinal window) (Figs. 4.2, 4.3) demonstrates the right aortic arch (asterisk) and an aortic diverticulum (arrowhead) (Fig. 4.2) giving rise to an aberrant left subclavian artery (arrow) (Fig. 4.3). Right Aortic Arch with Aberrant Left Subclavian Artery None Fig. 4.1 Fig. 4.2 Fig. 4.3 The aorta and great vessels develop from primitive paired dorsal aortas, which sequentially give rise to six paired primitive arches (Fig. 4.4), portions of which sequentially regress. The normal left aortic arch results from persistence of the left fourth primitive arch (Fig. 4.4), regression of the right fourth arch beyond the right subclavian artery, and persistence of the left dorsal aorta and the left ductus arteriosus (the latter forms from the left sixth primitive arch). The brachiocephalic, left common carotid, and left subclavian arteries arise in succession from the normal left aortic arch (Fig. 4.4). Right aortic arch affects approximately 0.1% of the population. A right aortic arch may exhibit mirror image or non–mirror image branching of the great vessels. In right aortic arch with mirror image branching, the left brachiocephalic, right common carotid, and right subclavian arteries arise in succession. The most common type of right aortic arch exhibits non–mirror image branching, and the left common carotid, right common carotid, right subclavian, and aberrant left subclavian arteries arise in succession. The aberrant left subclavian artery may be associated with dilatation of its origin (diverticulum of Kommerell). A coexistent left ligamentum arteriosus results in a complete vascular ring. Fig. 4.4
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


4 Right Aortic Arch