
Diagnosis: Submandibular duct sialolithiasis with sialadenitis
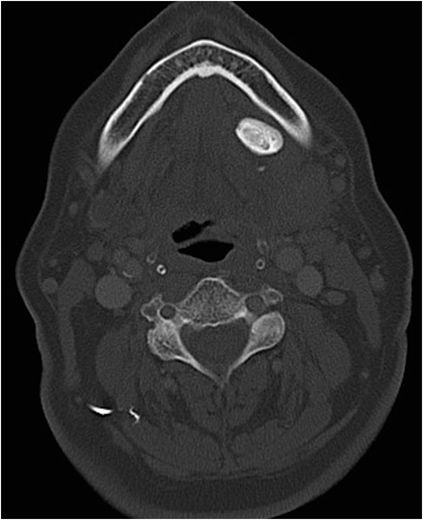
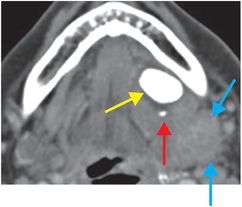
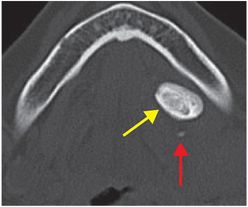
Noncontrast axial CT in soft tissue (left image) and bone windows (middle image) demonstrates a 2.1 cm radiopaque Wharton’s duct calculus (yellow arrows) in the left sublingual space between the extrinsic tongue musculature and left mylohyoid muscle with inflammation and effacement of adjacent fat. A smaller punctate calculus is seen within the more proximal aspect of the duct (red arrows). The left submandibular gland is enlarged and inflamed (blue arrows).
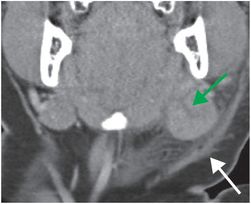
On coronal noncontrast CT (right image), the left submandibular gland is enlarged with internal dilated linear hypodensities representing dilated excretory ducts (green arrow). The right submandibular gland is normal. There is extensive inflammatory reticulation of the fat surrounding the submandibular gland and thickening of the platysma (white arrow).
Discussion
Overview of sialolithiasis
Sialolithiasis is the most common pathological condition affecting the salivary glands.
80 to 90 percent of cases involve the submandibular gland or duct (Wharton’s duct) while most remaining cases involve the parotid gland or duct (Stensen’s duct). Sublingual gland stones have been reported to occur rarely, in 1–7% of cases. In 25% of cases, stones are multiple.
This disease process most commonly affects adults in the 4th to 7th decades of life with a slight male predilection. Gout predisposes to the formation of uric acid stones that may not be seen on radiography but are clearly evident on CT.
The submandibular duct is thought to be the most common site of stones due to its long anatomical course, the narrow caliber of its orifice in comparison to the rest of the duct, and its relatively high salivary alkalinity and hydroxyapatite content. About 85% of submandibular stones are seen within Wharton’s duct and 15% are seen within the gland itself.
Clinical presentation and complications of sialolithiasis
Patients classically present with a history of recurrent facial swelling superficial to the affected gland that is worse with eating or gustatory stimulation.
Salivary transit is obstructed at the level of the stone resulting in proximal dilatation, stasis, and eventual glandular infection.
Abscess formation and deep cervical infection are known complications. Chronic obstruction may lead to duct strictures and fatty atrophy of the gland.
Rarely, an obstructing stone can cause salivary duct rupture and formation of an extravasating mucocele.
Anatomy of the salivary ducts
Detailed knowledge of the courses of the submandibular (Wharton’s) and parotid (Stensen’s) ducts is critical in evaluating for ductal calculi.
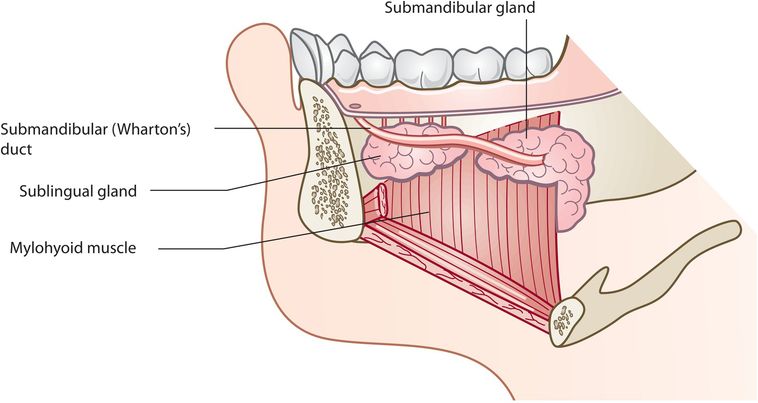
The submandibular (Wharton’s) duct courses through the sublingual space which is located between the mylohyoid muscle sling and extrinsic musculature of the tongue.
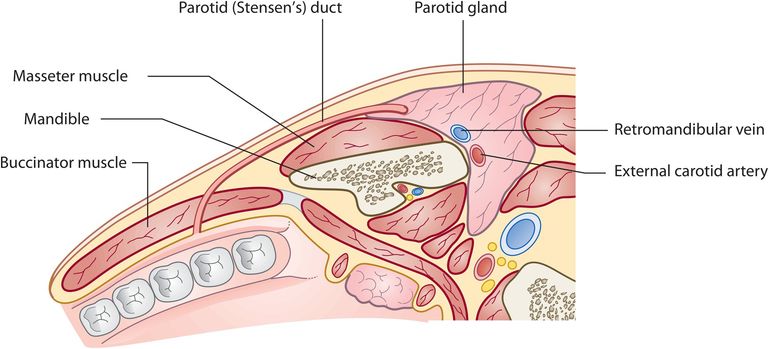
The parotid (Stensen’s) duct extends anteriorly from the parotid gland, running parallel to the masseter muscle within the buccal space. Along the anterior aspect of the masseter muscle, the duct courses medially, pierces the buccinator muscle and enters the oral cavity opposite the second upper premolar.
A calcific density along the course of either duct is a definitive sign of sialolithiasis.
Imaging of salivary gland stones
Most salivary gland stones are readily apparent on CT as they are composed of various radiographically dense calcium salts. On contrast-enhanced studies, small vessels in the sublingual space may mimic small calculi. With a severe enough degree of obstruction, the dilated duct may be seen as a tubular centrally hypodense structure.
In the setting of ductal infection, the fatty fascia surrounding the duct will appear infiltrated. Enlargement of the gland with surrounding inflammatory changes is typical of glandular infection. Peripherally enhancing, centrally hypodense areas within the gland or around the duct are suspicious for abscess formation.
MRI findings parallel those of CT. On T2-weighted images, stones appear as low-signal filling defects within the salivary duct, which is otherwise filled with high-signal saliva. The proximal duct may be dilated. An acutely inflamed or infected gland will exhibit high signal on T2-weighted images with fat suppression and low signal on T1-weighted images. In the setting of chronic obstruction, fatty infiltration of the gland appears as high signal intensity on T1-weighted and low signal intensity on T2-weighted images.
Although ultrasound may be useful to evaluate for sialolithiasis, image quality is highly operator-dependent and may be affected by the patient’s physical characteristics. High frequency transducers via an intra-oral approach have been found to be most effective with stones appearing as echogenic foci with posterior acoustic shadowing. If the duct is dilated, it typically appears as a tubular, anechoic structure proximal to the stone. In cases of severe obstruction, excretory ducts within the gland may also be dilated.
Related posts:
 12 68-year-old man with left lower quadrant pain and hypotension
12 68-year-old man with left lower quadrant pain and hypotension
 72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
 35 37-year-old woman with a history of rheumatoid arthritis presenting with non-resolving bilateral effusions and chest pain
35 37-year-old woman with a history of rheumatoid arthritis presenting with non-resolving bilateral effusions and chest pain
 62 38-year-old male complaining of diffuse abdominal pain after a motor vehicle collision
62 38-year-old male complaining of diffuse abdominal pain after a motor vehicle collision
 53 42-year-old female presenting with fever and back pain
53 42-year-old female presenting with fever and back pain
 66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


