CASE 41 A 72-year-old woman with known coronary artery disease (CAD) and prior myocardial infarction is referred for a dipyridamole myocardial perfusion PET study to evaluate nonanginal chest pain. Her cardiac risk factors include hypertension and known CAD. The resting ECG shows normal sinus rhythm, poor R-wave progression, and nonspecific T-wave abnormalities. She is on diltiazem, hydro-chlorothiazide, and aspirin at the time of testing. Fig. 41.1 • The patient had nothing to eat within 4 hours of the test. Caffeinated beverages were withheld for 24 hours before the test. • After a scout CT acquisition (120 kVp, 10 mA) for patient positioning, a CT transmission scan (140 kVp, 30 mA, pitch of 1.35) was acquired for attenuation correction. Commercial software was used for coregistration of the transmission and emission images. • A 60 mCi dose of 82Rb was administered at rest. • Resting images were obtained 90 seconds after completion of the radionuclide infusion for a total of 5 minutes. Resting gated images were acquired at 8 frames per cycle. • PET images were reconstructed with ordered subsets expectation maximization (OSEM; 2 iterations and 30 subsets), and a three-dimensional PET filter was used (Butterworth filter cutoff frequency of 10, order of 5). • Vasodilator stress was achieved with a standard intravenous infusion of dipyridamole (0.14 mg/kg per minute) for 4 minutes. • A 60 mCi dose of 82
Clinical Presentation
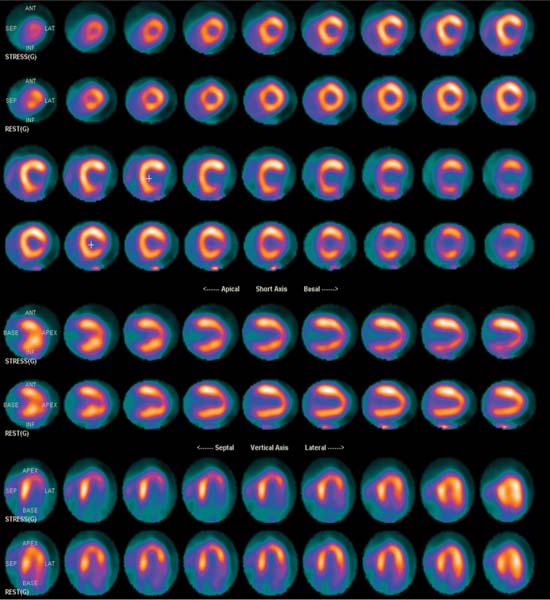
Technique
![]()
Stay updated, free articles. Join our Telegram channel





Full access? Get Clinical Tree


