CASE 42 A 74-year-old man with known coronary artery disease (CAD) and prior myocardial infarction (MI) is referred for a dipyridamole myocardial perfusion PET study for post-MI evaluation. Cardiac risk factors include hypertension and dyslipidemia. The resting ECG shows normal sinus rhythm and anterior and lateral Q waves. Medications include a β-blocker, an angiotensin-converting enzyme inhibitor, aspirin, a statin, and clopidogrel. Fig. 42.1 Fig. 42.2 • The patient had nothing to eat within 4 hours of the test. The β-blocker was withheld on the day of the test. Caffeinated beverages were withheld for 24 hours before the test. • After a scout computed tomographic (CT) acquisition (120 kVp, 10 mA) for patient positioning, a CT transmission scan (140 kVp, 30 mA, pitch of 1.35) was acquired for attenuation correction. Commercial software was used for coregistration of the transmission and emission images. • Rest emission images were obtained for 5 minutes after the intravenous administration of 60 mCi of 82Rb at rest, with imaging starting 120 seconds (given the low ejection fraction) after completion of the radionuclide infusion. Rest gated images were acquired at 8 frames per cycle. • PET images were reconstructed with ordered subsets expectation maximization (OSEM; 2 iterations and 30 subsets), and a three-dimensional PET filter was used (Butterworth filter cutoff frequency of 10, order of 5). • Vasodilator stress was achieved with a standard intravenous infusion of dipyridamole (0.14 mg/kg per minute) for 4 minutes. • The patient was injected with 60 mCi of 82
Clinical Presentation
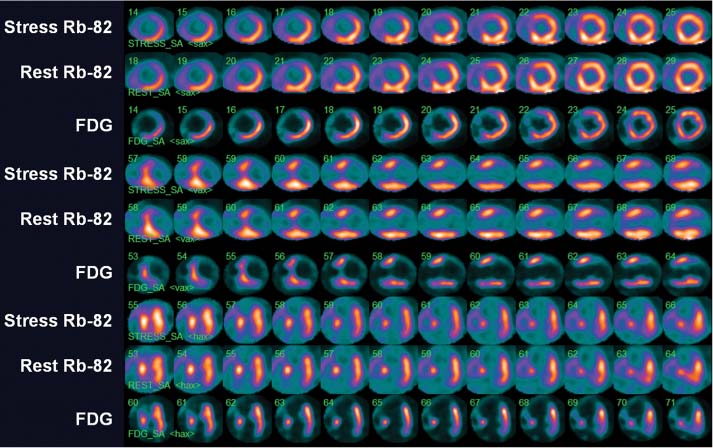
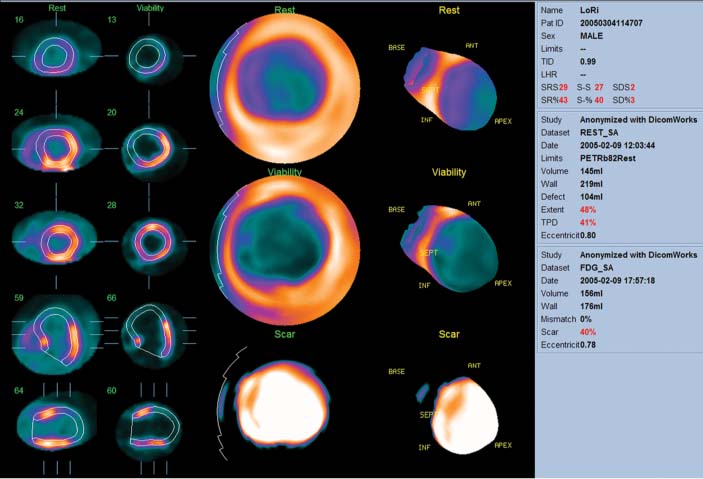
Technique
![]()
Stay updated, free articles. Join our Telegram channel




Full access? Get Clinical Tree


