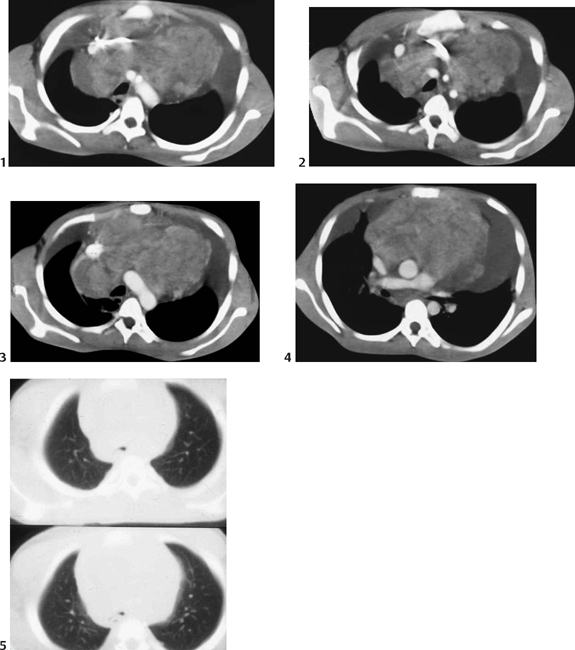
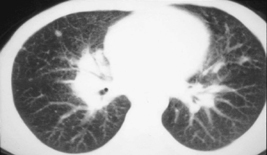
CASE 43 A 14-year-old presents with 2 weeks of intermittent fever and swollen neck nodes on the right. Figure 43A Initial frontal (Fig. 43A1) and lateral (Fig. 43A2) chest radiographs demonstrate a large anterior mediastinal mass causing posterior tracheal compression and deviation. A moderate-sized left pleural effusion is present. Multiple axial CT postintravenous contrast enhancement scans (Figs. 43B1 to 43B4) demonstrate a large anterior mediastinal mass. This bulky, inhomogeneous, and nodular mass causes vascular deviation and significant superior vena cava (SVC) compression. Note that the left pleural effusion is located anterior, as the child was scanned in the prone position due to respiratory compromise when in the supine position. Images using lung windows (Fig. 43B5) demonstrate significant tracheal narrowing. Figure 43B Hodgkin’s lymphoma Figure 43C Axial slice at lung windows from a CT scan demonstrates a fine interstitial process of lymphatic dilatation, which could be secondary either to central lymphatic obstruction by the tumor or to interstitial spread of tumor into the lung through lymphatic channels. A nodule in the right middle lobe is in keeping with parenchymal involvement with lymphoma. Lymphoma, the third most common malignancy in children behind leukemia (first) and CNS tumors (second), constitutes approximately one quarter of all pediatric mediastinal masses. The most common anterior mediastinal mass in children is the nodular sclerosing subtype of Hodgkin’s disease. Approximately 85% of children with Hodgkin’s disease have involvement of the intrathoracic lymph nodes, whereas 60% of children with non-Hodgkin’s have intrathoracic/mediastinal nodal involvement.
Clinical Presentation
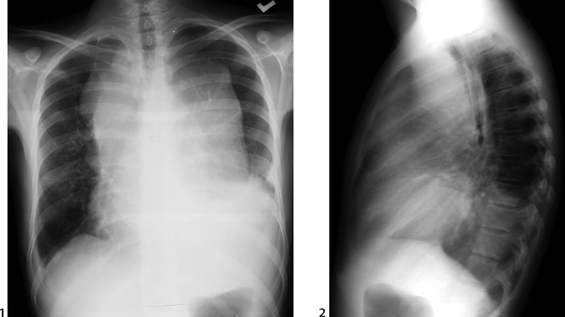
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Clinical Findings
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


