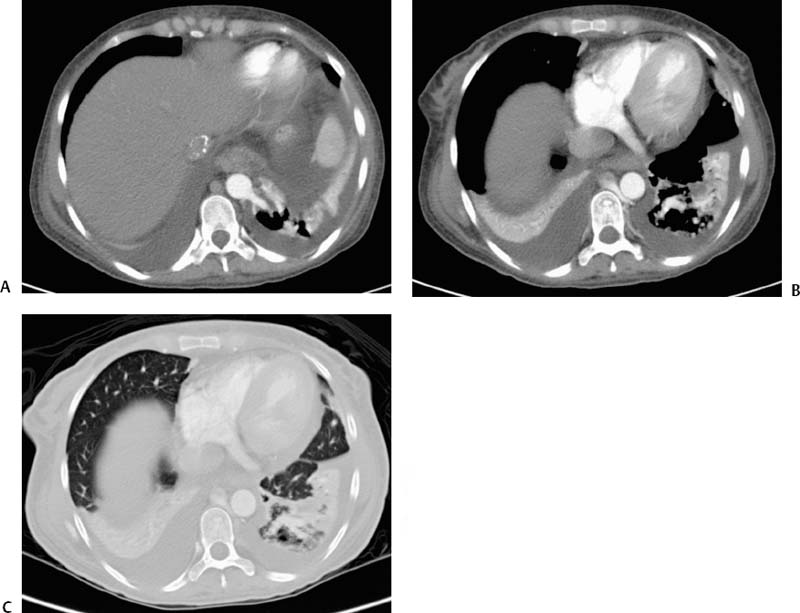
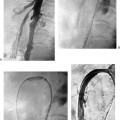
CASE 56 A 16-year-old female hospitalized for complications related to her second liver transplant underwent cultures and chest radiography for evaluation of fever of unknown origin. Radiographic findings (Fig. 56-1) were suspicious for pneumonia and were similar to those seen on previous admissions. Blood and sputum cultures were negative. Figure 56-1 A 16-year-old female status post liver transplant was evaluated for fever of unknown origin. Chest radiography shows ill-defined opacity in the left lower lobe. Plain chest radiography revealed a chronic, retrocardiac opacity, not significantly changed during the previous year. CT and MRI (Figs. 56-2 and 56-3) showed an ill-defined enhancing area in the left lower lobe with cystic and solid components. A large branching vessel originating from the aorta supplied this area. Aortography (Fig. 56-4) showed two large aberrant vessels originating from the aorta to supply a region of marked hypervascularity in the left lower lobe. No early draining vein was visible. Venous drainage was via the azygous system. Extralobar bronchopulmonary sequestration. The patient’s fevers were determined to be the result of transplant graft rejection, and she was considered to have an asymptomatic extralobar sequestration (ELS). Given her history of multiple major abdominal operations, the risks of additional surgery were weighed against the potential future complications of an ELS. No treatment was performed, and the patient has remained asymptomatic from the sequestration for 4 years. Figure 56-2 Arterial phase axial CT images. (A) A large aberrant branch of the aorta extends into the left lower chest. (B) The aberrant artery branches to supply an inhomogeneous, partially cystic, partially solid mass. (C) Lung windows show emphysematous changes in the left lower lobe surrounding the mass. Contrast material Micropuncture set (Cook, Bloomington, Indiana) 0.035″ standard guidewire (Boston Scientific, Natick, Massachusetts) 5F angiographic pigtail catheter (Boston Scientific, Natick, Massachusetts) 5F Visceral Selective catheter (RC-1; Boston Scientific, Natick, Massachusetts)
Clinical Presentation

Radiologic Studies
Diagnosis
Treatment
Equipment
Discussion
Background
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


