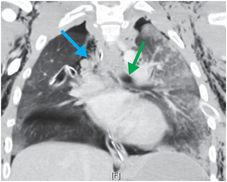
Diagnosis: Traumatic laceration of the right mainstem bronchus with pneumothorax and “fallen” lung
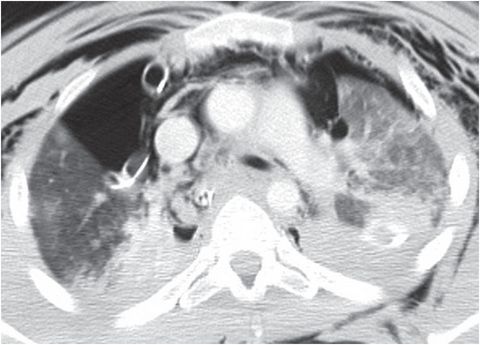
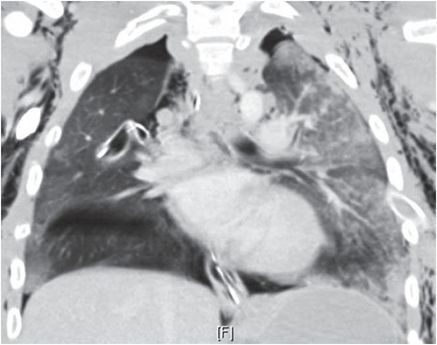
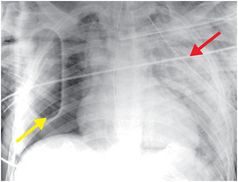
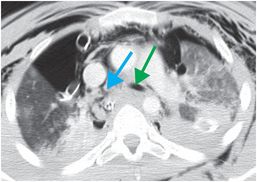
A portable chest radiograph shows extensive subcutaneous emphysema, the “visceral pleural line” sign of a right pneumothorax (yellow arrow), bilateral chest tubes, and a left upper lobe contusion (red arrow). Axial and coronal enhanced CT images also demonstrate extensive pneumomediastinum, bilateral pneumothoraces and pulmonary contusions, and narrowing and irregularity of the right mainstem bronchus (blue arrows); for comparison, note the normal contour and caliber of the left mainstem bronchus (green arrows). The right lung has fallen dependently towards the posterior chest wall despite placement of a chest tube.
Discussion
Thoracic injuries are the third most common type of injury in trauma patients (after head and extremity injuries) and are implicated in approximately one-quarter of trauma-related deaths.
Motor vehicle accidents are the mode of injury in more than two-thirds of cases of blunt thoracic trauma.
Injuries to the heart and tracheobronchial tree carry the highest mortality of all injury types in blunt thoracic trauma.
In patients with suspected thoracic trauma, radiography is generally the modality of choice for initial evaluation; however, CT often reveals injuries even with normal radiographs.
Radiographs facilitate identification of life-threatening injuries that require immediate attention, such as tension pneumothorax, hemothorax, mediastinal hemorrhage, and support line and tube misplacement. Superimposed objects (e.g., trauma boards and EKG leads) and suboptimal positioning of injured patients may complicate interpretation of portable radiographs.
Chest CT images should be systematically interpreted in soft tissue windows (for evaluation of the heart, vasculature, esophagus, pleural collections, and the chest wall), lung windows (for evaluation of the lung parenchyma and tracheobronchial tree), and bone windows (for evaluation of the ribs and thoracic spine).
IV contrast is recommended unless there is a known contraindication (such as allergy or known renal insufficiency). Water-soluble enteric contrast such as Gastrografin may be considered in cases with suspected esophageal injury.
Multiplanar reformatted images are generally very useful in the evaluation of thoracic injury. 3D and MIP reconstructions are sometimes useful in the evaluation of complex cardiovascular and bone injuries, while minimum intensity projection (miniP) reconstructions are occasionally useful in the evaluation of airway injuries.
Ultrasound may be used at the bedside for evaluation of the heart, pericardium, and pleural space. MRI currently does not play a role in the management of thoracic trauma.
| Lung |
|
| Pleura |
|
| Heart and vessels |
|
| Thoracic cage |
|
| Other |
|
Clinical synopsis
Large air leak from the right chest tube, along with the imaging findings of a fallen right lung and massive subcutaneous emphysema, raised concern for a tracheobronchial laceration. The patient underwent bronchoscopy, which demonstrated a circumferential tear of the right mainstem bronchus below the carina. The patient recovered uneventfully after urgent right thoracotomy and repair of the right mainstem bronchus.
Related posts:
 12 68-year-old man with left lower quadrant pain and hypotension
12 68-year-old man with left lower quadrant pain and hypotension
 72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
 35 37-year-old woman with a history of rheumatoid arthritis presenting with non-resolving bilateral effusions and chest pain
35 37-year-old woman with a history of rheumatoid arthritis presenting with non-resolving bilateral effusions and chest pain
 62 38-year-old male complaining of diffuse abdominal pain after a motor vehicle collision
62 38-year-old male complaining of diffuse abdominal pain after a motor vehicle collision
 53 42-year-old female presenting with fever and back pain
53 42-year-old female presenting with fever and back pain
 66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


