

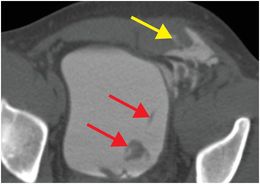
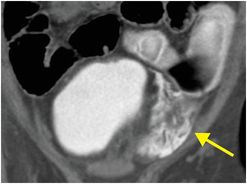
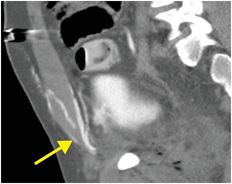
Diagnosis: Extraperitoneal bladder rupture
Axial (left image), coronal (middle image), and sagittal (right image) CT cystogram (with some enteric contrast from a previous examination) demonstrates contrast extravasation from the distended bladder into the extraperitoneal space (yellow arrows) and superficial soft tissues, consistent with a complex extraperitoneal bladder rupture. Filling defects (red arrows) within the bladder likely represent blood clots.
Discussion
Imaging and classification of bladder injuries
Evaluation of bladder injuries may be accomplished by CT cystogram or conventional cystography, which require retrograde filling of the bladder with 300–400 mL of diluted contrast material by gravity. The bladder must be adequately distended to reliably detect wall disruption. Identifying the site of contrast extravasation is important in localizing the site of rupture. In many trauma centers, CT cystography has supplanted conventional cystography as the preferred modality.
Accurate classification of bladder injuries is essential in guiding management in the trauma setting. Bladder injuries can be classified into five types based on cystography findings:
Type 1: Bladder contusion resulting from an incomplete tear in the bladder mucosa. Imaging findings may be normal or simply show mild focal wall thickening.
Type 2: Intraperitoneal rupture, most commonly occurring at the bladder dome as a result of blunt trauma to a distended bladder. There is increased risk for chemical peritonitis. Conventional and CT cystography findings include contrast extravasation into the peritoneal cavity. Contrast is often most visible in the paracolic gutters and between loops of small bowel.
Type 3: Interstitial injury resulting from a tear of the serosal surface. This is rare, and imaging findings include a mural defect without contrast extravasation. There may be intravasation of contrast within the bladder wall.
Type 4: Extraperitoneal rupture often occurs anterolaterally near the base of the bladder and is usually associated with pelvic fractures. Conventional and CT cystography findings of extravasation into the extraperitoneal space of Retzius are classified as simple, or Type 4A. With extension into the scrotum, perineum, and thigh, extraperitoneal rupture is classified as complex, or Type 4B.
Type 5: Combined intraperitoneal and extraperitoneal bladder rupture.
Treatment of bladder injuries
Bladder contusions (Type 1) and interstitial injuries (Type 3) are treated conservatively, with urinary diversion by Foley catheter placement.
Intraperitoneal ruptures (Type 2) and combined intra- and extraperitoneal ruptures (Type 5) are treated with surgical repair.
Extraperitoneal ruptures (Type 4) may be treated conservatively with urinary diversion unless the bladder neck is injured, in which case surgical intervention may be required.
Clinical synopsis
The patient was treated conservatively with Foley catheter placement until the urine cleared of blood. Surgical intervention was not required in this case.
Self-assessment
Related posts:
 12 68-year-old man with left lower quadrant pain and hypotension
12 68-year-old man with left lower quadrant pain and hypotension
 72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
 35 37-year-old woman with a history of rheumatoid arthritis presenting with non-resolving bilateral effusions and chest pain
35 37-year-old woman with a history of rheumatoid arthritis presenting with non-resolving bilateral effusions and chest pain
 62 38-year-old male complaining of diffuse abdominal pain after a motor vehicle collision
62 38-year-old male complaining of diffuse abdominal pain after a motor vehicle collision
 53 42-year-old female presenting with fever and back pain
53 42-year-old female presenting with fever and back pain
 66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


